Introduction
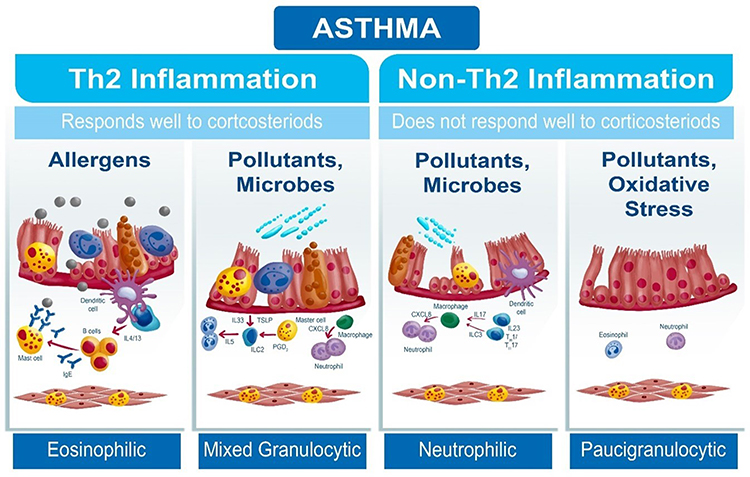
Asthma in the pediatric population is present in about one in every 10 children and adolescents around the world, presenting heterogeneous characteristics composed of different clinical phenotypes and endotypes.1,2 The underlying cellular and molecular mechanisms (endotypes) of asthma have been represented by Th2 and non-Th2 inflammatory patterns. The Th2 inflammatory pattern, which responds well to the use of inhaled corticosteroids (ICS), accounts for approximately 50 to 60% of asthma in the pediatric population. In this spectrum of inflammation, allergic eosinophilic asthma is the most prevalent in children and adolescents, in which environmental allergens become real villains.3
On the other hand, the non-Th2 inflammatory pattern represents a significant and growing number of patients who do not respond well to the use of IC and are classified as having neutrophilic or paucigranulocytic asthma (Figure 1). In non-Th2 inflammation, the allergic components are not present in the patient and the immune responses are triggered mainly by the stimulus of pollutants and inhaled irritants, with an important participation of type 1 helper T cells (Th1) and 17 (Th17), in addition to pro-inflammatory interleukins such as IL-17, IL-25, IL-33 and thymic stromal lymphopoietin (TSLP).4
 |
Figure 1 Participation of pollutants and inhaled irritants in inflammation of the respiratory epithelium in different asthma endotypes.
|
In the hypothesis of the epithelial barrier, the inflamed bronchial mucosa becomes hyper-reactive to various stimuli, whether allergic or not, which can trigger episodes of asthma exacerbations. Among the environmental risk factors, allergens stand out, represented mainly by house dust mites, dog and cat hair, cockroaches, fungi, pollens, among other well-known triggers of asthma exacerbations.5
Growing interest has been focused on pollutants and inhaled irritants present in the home, inside or adjacent to the internal space of the residence, which can harm the respiratory tract and trigger clinical worsening of asthma. Tobacco smoke, use of charcoal stoves, firewood, gas stoves, particulate matter, volatile substances from chemicals used in household cleaning or swimming pool cleaning, use of pesticides, among many, often forgotten, but which may be present in the home environment and need to be detailed in the clinical history of every patient with or without allergic asthma.6,7
The environment to which the individual is exposed (exposome) continuously influences the clinical control of asthma. The exposome concept considers an individual’s environmental, behavioral, and lifestyle exposures over a lifetime and how these exposures relate to health. In the context of asthma, there are well-known associations, associations that are not fully established, and exposures that demonstrate more distinct effects based on age, chronicity of exposure, and genetic predispositions.8
Health professionals become the first link in the investigation of environmental factors and how they impact the pathogenesis, symptoms, evolution and morbidity of asthma. When it comes to asthma in the pediatric population, a complex disease with an important gene-environment interaction, the caregiver’s role in the home environment becomes essential.9 Under Antonovsky ‘s salutogenic view, the caregiver represents the most effective agent in promoting home environmental control to avoid both allergic sensitization and asthma exacerbation crises.10
The central concept of Antonovsky ‘s Salutogenic theory is called sense of coherence (SOC), an individual construct that influences habits that directly interfere with health and adaptive behaviors that can minimize the severity of diseases. The SOC has three main components: the ability to understand an event (comprehensibility), the perception of the potential to manipulate or solve it (manageability) and the meaning given to this event (significance). It consists of a global orientation towards seeing life as structured, manageable and with an emotional meaning.11
The Salutogenic theory (saluto = health; genesis = origin) proposed in 1979, by Antonovsky – Israeli American sociologist and professor, states that health-promoting factors have a direct impact on the patient’s quality of life. Its assumptions consider health as a result of the adaptive capacity of human beings in the face of life’s adversities.12 When it comes to home environmental control, the caregiver becomes a key player in preventing and controlling exposure to inhaled products and substances that can alter the clinical control of asthma.
In this context, it is important for health professionals to identify and guide caregivers about the likelihood of certain pollutants and irritants in the home inhalation triggering clinical worsening of asthma. Therefore, this integrative review proposes to present the most common and frequent pollutants or inhalation irritants that can be found in the home environment, highlighting their possible repercussions in the worsening of health through aggression to the respiratory epithelium and consequent impairment of lung function in pediatric patients with asthma, and in this context, highlight the caregiver’s role - through the salutogenic perspective - as a modifying agent for adequate environmental control.
Materials and Methods
Selection Criteria
The research was carried out in the databases MEDLINE/PubMed, Latin American and Caribbean Literature in Health Sciences (Lilacs), Web of Science and Scopus, with the objective of describing the pollutants and inhalant irritants most found in the home environment, their possible repercussions on the respiratory epithelium and lung function that can worsen health and worsen the clinical control of asthma in the pediatric population. The sense of coherence of the salutogenic theory has been investigated in studies directed at asthma and other diseases.
Search Strategy
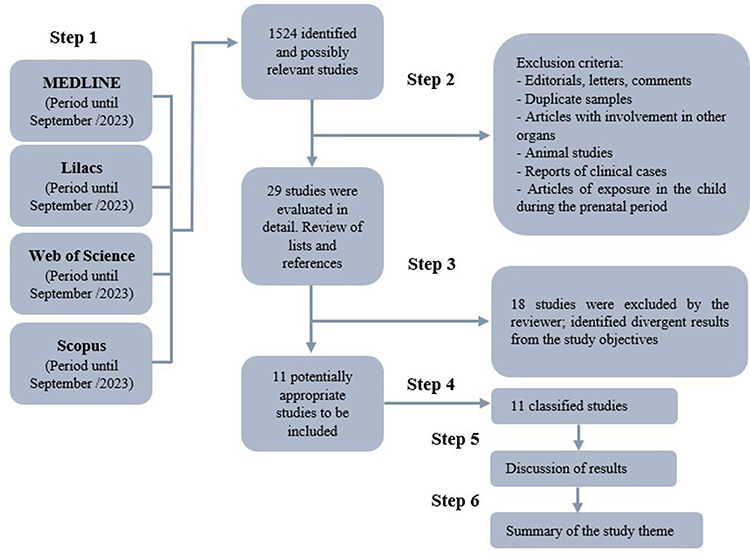
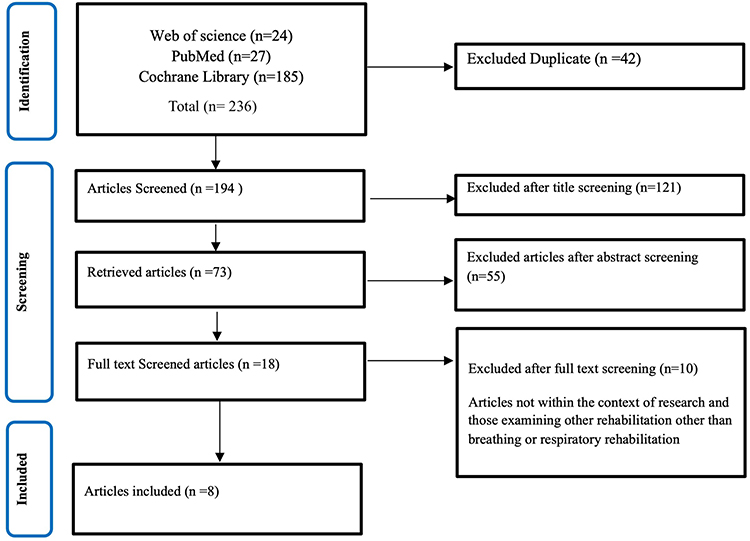
The following descriptors were used: air pollution AND asthma OR/AND lung function; irritants AND asthma; tobacco AND asthma AND pulmonary function; particulate matter AND asthma; disinfectants AND asthma OR/AND lung function; hydrocarbons, fluorinated AND asthma; odorants AND asthma; chloramines AND/OR pool AND asthma; pesticide AND asthma AND lung function; Antonovsky ‘s sense of coherence. The inclusion criteria used for the research were: observational or experimental articles related to the repercussions of pollutants and inhaled irritants on the respiratory tract in humans, in addition to review articles that were published in the last 10 years, in English and Spanish, searched up to September 2023; and a textbook on the sense of coherence of Antonovsky ‘s salutogenic theory (Figure 2).
 |
Figure 2 Article search strategy flowchart.
|
This article is focused only on pollutants and irritants of an inhalation nature, which can be frequently identified in any household and which have a potential deleterious effect on the respiratory tract. It highlights, therefore, the main products found, properties of action and possible repercussions in the worsening of health, especially in asthma, but it does not intend to be an exhaustive review on the subject.
Publications such as comments, editorials, letters, studies with results from other affected organs other than the respiratory tract, studies that projected exposure effects on the child during the mother’s prenatal period, animal studies, case reports and duplicate articles were excluded. After sorting by reading the titles and abstracts evaluated by the reviewer (G.V.A.G.L.), the full reading began, with more articles being included through manual search, through the references of the initially pre-selected studies on the subject. Although animal studies were not included, studies of some substances in the respiratory tract of animals may have been cited to better elucidate the pathogenic mechanisms of inflammation in asthma.
Which Pollutants and Irritants in the House May Aggravate the Health of Patients with Asthma?
Early identification and removal of polluting particles and inhaled irritants, especially in the home environment, are effective ways to maintain health and prevent asthma exacerbations. The lungs are structures widely exposed to ambient air, with approximately 100 square meters of surface area in contact with the outside world, compared only to the skin in terms of the intensity of environmental exposure. With each respiratory movement, various particles, gases and microorganisms transit between the ambient air and the alveoli, which may cause sensitization or damage to the respiratory epithelium.13
Allergic tests can identify sensitization to inhaled antigens and their correlation with the clinic define an allergic pattern in the individual. Negative tests, therefore, are useful to exclude an allergic basis for asthma and it is in this context that the environmental recall becomes even more essential to identify substances and inhaled particles, present in the home, that can trigger symptoms and exacerbation crises of asthma. Asthma in the pediatric age group, a period totally susceptible to the care of a caregiver responsible for environmental control.14,15
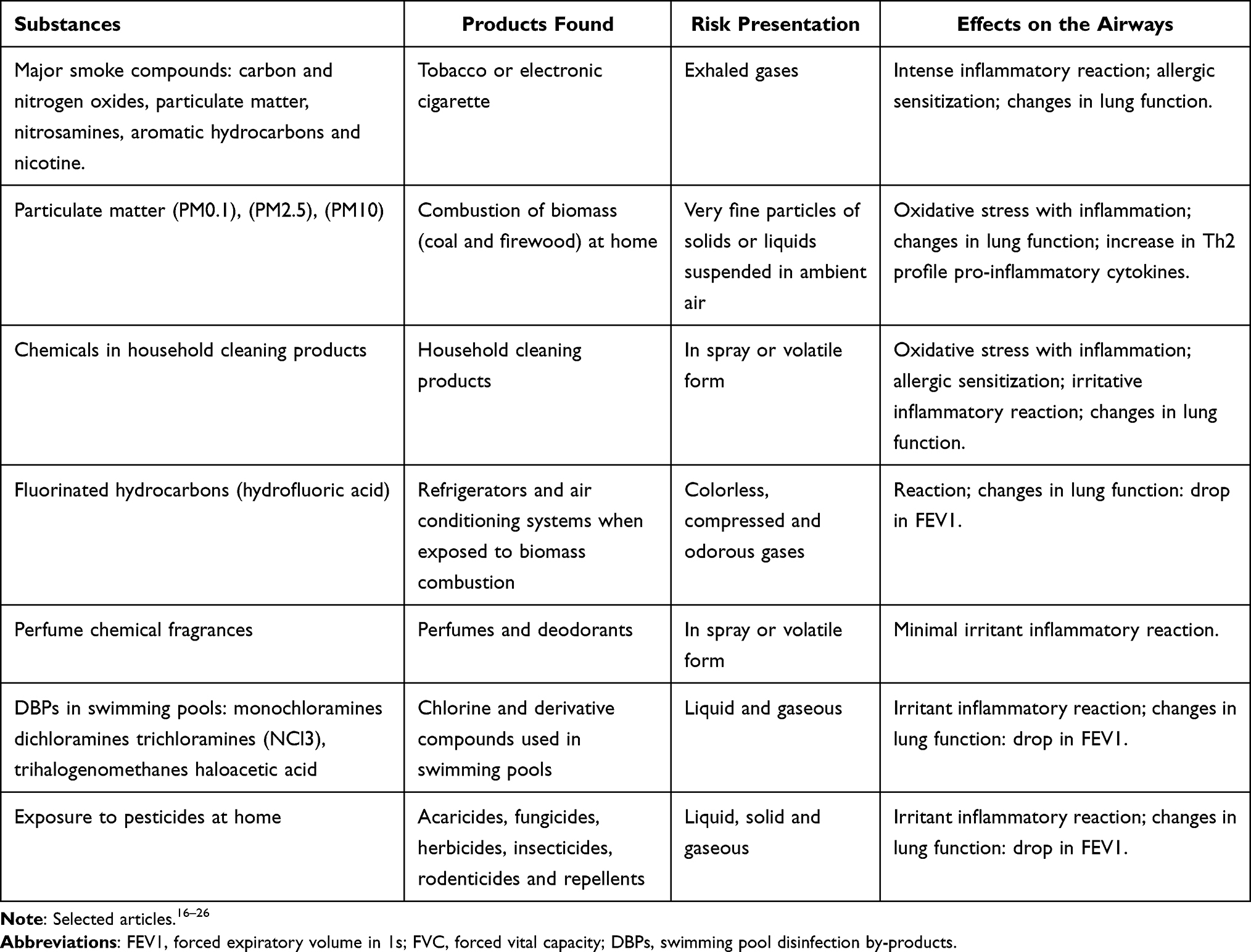
Substances and inhaled products that can be found in the home environment should be identified by health professionals who care for patients with asthma in the pediatric age group, to better guide caregivers on what should be avoided to protect the patient’s health. Below, the seven main and most common products considered irritants and pollutants inhaled at home, which can worsen the patient’s respiratory health, will be listed and commented on (Table 1).16–26
 |
Table 1 Substances Identified in the Home Environment That Can Affect the Airways
|
Secondhand Smoke Exposure in the Pediatric Population
Secondary exposure to environmental tobacco, cigar, or e-cigarette vapors has been associated with increased chances of exacerbations and lack of clinical control of asthma. Effects of pre- or postnatal tobacco smoke constitute one of the most important risk factors for childhood asthma, leading to alterations in lung development, even in utero, and in immunological and epigenetic responses that favor asthma.27,28
Tobacco smoke, now so well known, is a mixture of compounds including carbon and nitrogen oxides, particulate matter, nitrosamines, polycyclic aromatic hydrocarbons, carbonyls, and numerous other chemicals, many of which are known toxicants that can induce inflammation and responses altered immune. Among these compounds, nicotine and its metabolites are the most responsible for chemical dependence and deleterious effects on the lungs, such as intense inflammatory reaction, allergic sensitization and changes in lung function.29
Negative health outcomes are not limited to indoor smoking, but also the continued elimination of tobacco compounds from people who smoked outside the home. In addition, residues from tobacco smoke, known as third-hand smoke, can persist for weeks to months in the home, adhering to surfaces and house dust after the smoke has evaporated. The residue is composed of chemicals that can react with other atmospheric pollutants, forming volatile toxic particles.30
Nicotine metabolites, such as cotinine, have been used as an objective measure of passive exposure in epidemiological studies. Self-reported measurements of exposure to secondhand smoke did not show good specificity when compared to measurements of plasma cotinine. In fact, approximately 41% of children whose parents reported in the clinical history that they were not active smokers in the household had detectable levels of plasma cotinine, with mean plasma cotinine levels increasing as the number of household smokers increased.16
On the other hand, the use of electronic cigarettes has been replacing the use of conventional cigarettes and has been increasingly used by adolescents. Recent findings suggest that e-cigarettes, also known as e-cigs, electronic nicotine delivery devices, e-vaporizers or vapers, can cause respiratory damage in a similar way to traditional cigarettes and still pose other risks to users and passive inhalants.31
Vapers are devices that have a battery, an atomizer and a tank or cartridge to contain the e-liquid composed of propylene glycol and vegetable glycerin, in addition to several other compounds of common cigarettes, which when they decompose form carbonyl compounds with known inhalation toxicity and irritating properties to the respiratory epithelium. Other harmful compounds are liquid flavorings, such as diacetyl (2,3-butanedione), which can cause irreversible lung disease.32
Flavoring agents with potential respiratory hazards due to possible volatility and respiratory irritant properties are: acetoin, camphor, and cyclohexanone (minty flavor), benzaldehyde (cherry or almond flavor), cinnamaldehyde (cinnamon flavor), cresol (leather or medicinal flavor), butyraldehyde (chocolate flavor) and isoamyl acetate (banana flavor).33
Although smoking cessation is the most appropriate strategy, this has not been shown to be a intervention, as it depends on the cooperation of the smoker’s family members. Smoking outside the home may not be an effective mitigation strategy due to the residual risk of smoking.34 It is important to advise caregivers to stop smoking and keep the home environment free of tobacco smoke, cigars or electronic vaporizers, as the health risks are serious and passive smoking has been associated with a worse clinical outcome of asthma in childhood and adolescence.
Particulate Matter (PM) Indoors
Particulate matter (PM) can be formed by solid or liquid particles that remain in air suspension invisibly, different from large particles, which can be visible with appropriate lighting, such as fog or dust. These particles can be organic chemical compounds, acids such as sulfates and nitrates, metals and even dust. PMs are identified by their aerodynamic size or diameter: PM0.1 is < 0.1µm in diameter, PM2.5 is < 2.5µm and PM10 is < 10µm in diameter and are commonly emitted from combustion sources.35
The fine particles (PM2.5) manage to reach the pulmonary alveoli, where they will be captured by local cells and transported by the bloodstream, whereas the finer particles (PM0.1) pass through the alveolar-capillary membrane and confer greater systemic toxicity. In many parts of the world, smoking, incense burning, candles and mosquito coils are the main sources of PM2.5 indoors, where poor ventilation in homes can lead to extremely high levels of indoor pollution and deterioration of the environment lung function.36
The burning of incense for religious ceremonies or to perfume the air at home, in addition to the burning of repellents to eliminate mosquitoes, have generated toxic pollutants that have been associated with alveolar oxidative damage, respiratory diseases and even lung cancer.20
Particles resulting from the combustion of fossils, especially from the combustion of biomass (coal) used in home cooking, contain many heavy metals on their surfaces, such as arsenic, lead, cadmium or compounds such as sulfuric acid or cyclic aromatic hydrocarbons, which can be captured during the combustion process and transported on the surface of finer particles (PM2.5) to the pulmonary alveoli. Although the world still depends on biomass fuel for cooking and heating, it is known that public policies for environmental control are still limited. The use of firewood or coal for residential cooking and heating, in poor and cold geographic regions, has become frequent, especially in low-income countries.7
Natural gas is a popular fuel choice for home cooking. Among all gas appliances, stoves, cooktops and ovens in homes have their particularities, because combustion by-products are emitted directly into the domestic air, such as methane gas, formaldehyde (CH2O), carbon oxide (CO) and nitrogen oxides (nitric oxide - NO and nitrogen dioxide - NO2) and cause oxidative stress with inflammation, changes in lung function and a significant increase in Th2 profile pro-inflammatory cytokines.26
Repercussions on the respiratory tract can be observed even in early but intense phases of exposure to these materials suspended in the air. PM can also lead to chronic local inflammation and even pulmonary fibrosis in prolonged exposures. When there is overload of the macrophage function and the cells of the respiratory epithelium are exposed, oxidative stress is triggered and a cascade of inflammatory events, with production of cytokines IL-25, IL-33, TSLP, become evident.36
Special consideration is also being given to microplastics (PMs), which have a diameter of less than 0.5 cm and can be found in the air, indoors. The main sources of PMs for indoor air can be identified in textile products (clothes, curtains, mattresses), toys, rubber materials, kitchen utensils (plates, cups, bowls, bottles), electrical cables, electronics, indoor paint and cleaning agents, with a higher concentration in bedrooms.37
Inhalation is the main route of human exposure to microplastics and their accumulation in the human airways can cause inflammatory and immune responses in the lung interstitium due to the cytotoxic effect of the particles. Oxidative stress with repercussions on lung function are the main results of respiratory epithelial damage.38
Guidance for caregivers should emphasize the importance of having a ventilated home environment, with windows, preferably in urban areas free of burning garbage or biomass close to housing, clarify the risks that cooking indoors can bring to children’s lungs asthmatic and responsible. Alternatives such as having charcoal stoves outside the home, in the open air, or in ventilated residential annexes, can reduce exposure to particulate matter, especially in low-income populations.39
Substances in Household Cleaning Products
There are a variety of cleaning products and quantitative assessments of their presence in the air are challenging because these products are complex mixtures of chemicals that require different sampling methods and analytical measurement.40
Chemicals that require the most attention in relation to respiratory effects in asthma are corrosive ones, such as strong acids and bases (including ammonia and hypochlorite) and quaternary ammonium compounds. Solvents, including glycols and glycol ethers, as well as propellants, which are generally weak lower airway irritants, can potentiate the effects on the respiratory epithelium, especially if they are mixed in the same cleaning product.41
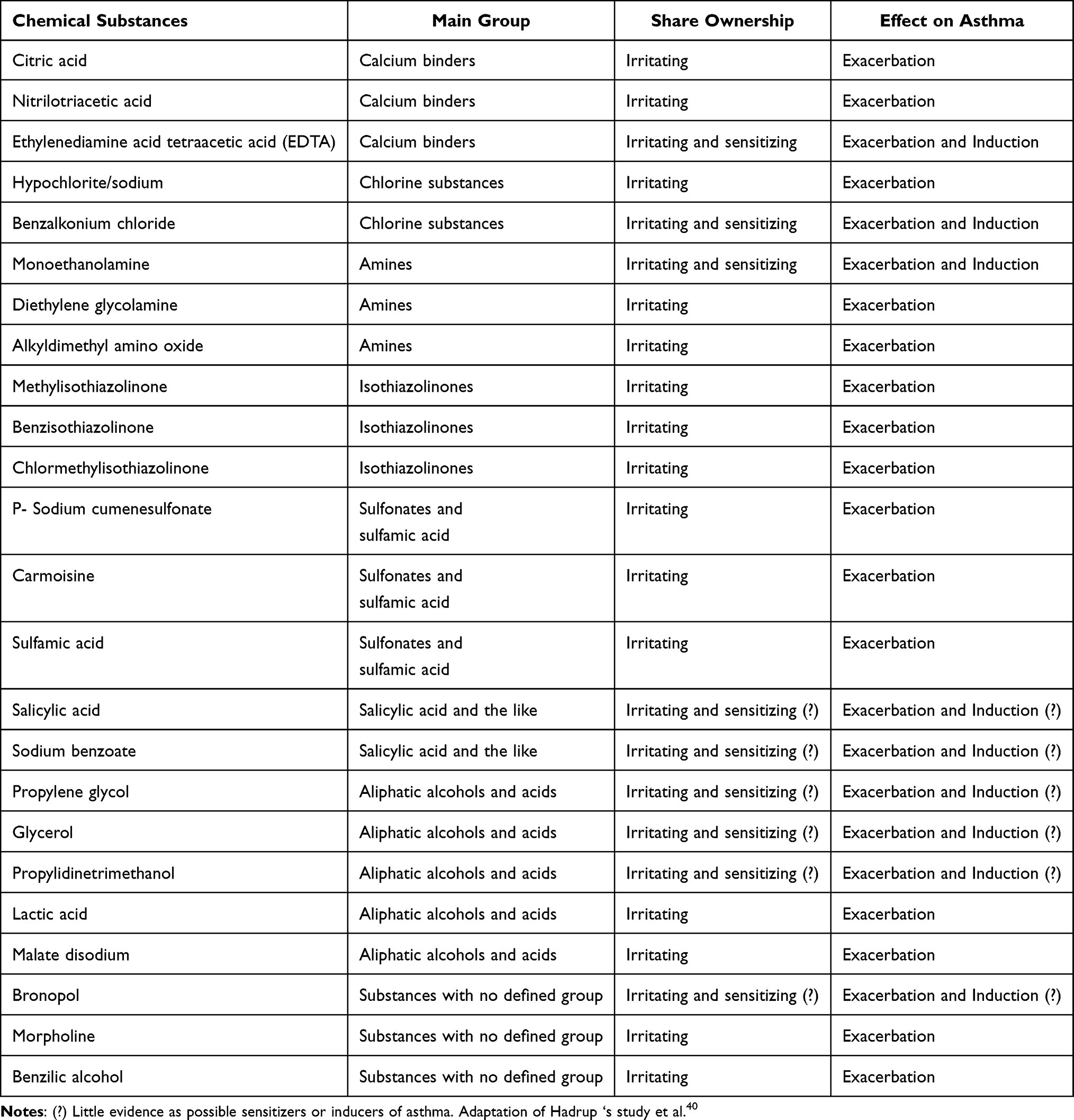
In Table 2, the chemical substances are presented according to the main molecular group, properties of action and risks of exacerbation or induction of asthma in people who may be exposed during household cleaning. We identified 24 substances that are more present in general cleaning products in spray or volatile form and that exert an irritating mechanism on the respiratory epithelium; three substances have the potential to sensitize asthma (benzalkonium chloride, ethylenediamine acid tetraacetic – EDTA and monoethanolamine); and six substances (salicylic acid, sodium benzoate, propylene glycol, glycerol, propylidinetrimethanol and bronopol) have little evidence as possible sensitizers in asthma.40,42
 |
Table 2 Characteristics of Chemical Substances Found in Residential Cleaning Products
|
More than 95% of volatile household cleaners contain chemicals that can irritate the respiratory epithelium. For example, sanitizers, considered disinfectants and degreasers, may contain citric acid, nitrilotriacetic acid, ethylenediamine acid tetraacetic acid (EDTA), benzalkonium chloride, monoethanolamine, diethylene glycolamine, alkyldimethyl amino oxide, methylisothiazolinone, benzisothiazolinone, chlormethylisothiazolinone, sodium benzoate, propylene glycol, glycerol, propylidinetrimethanol, lactic acid, malate disodium and salicylic acid. Liquid waxes for illustrating furniture and floors may contain bronopol and morpholine. Cleaning products that give off fragrance may contain benzyl alcohol. Descalers may contain sulfamic acid, and disinfectants and bleaches may contain sodium hypochlorite, sodium p- cumenesulfonate, and carmoisine.40
Guidance on avoiding the use of cleaning products or spray preparations containing mainly benzalkonium chloride and EDTA is important to prevent the induction or worsening of asthma, especially for those patients who are under the care of a guardian and are vulnerable to the dynamics cleaning in the residential environment. If the use of these spray preparations is not prohibitive, guidance can be given on keeping children with asthma away from home during the cleaning period at home and on the use of a mask by the caregiver. The recommendation for caregivers is that these products can be replaced or that the limitations of using these substances, especially in sprays, in closed environments be informed.43
Fluorinated Hydrocarbons
Chlorofluorocarbons (CFCs) and hydrochlorofluorocarbons (HCFCs), known as freons, were used as refrigerants until the early 2000s. Due to their ozone-depleting properties, freons have increasingly been replaced by chlorine-free refrigerants such as fluorinated hydrocarbons.44
Fluorinated hydrocarbons, which can thermally degrade to toxic hydrofluoric acid, are widely used as cooling agents in air conditioning systems, refrigerators, and as propellants in some medical aerosols. When fluorinated hydrocarbons are used in the presence of combustion, thermal degradation can lead to the formation of hydrofluoric acid, which is a known causative agent of irritant-induced asthma. Therefore, combustion sources, such as fireplaces, can be a risk for those using air conditioning in closed rooms and in confined residential environments.21
Hydrofluoric acid is associated with chemical pneumonitis, especially after exposure indoors, resulting from the combustion of fluorinated hydrocarbons, causing respiratory symptoms and changes in lung function after months of exposure. Guidance for caregivers, as providers of home security and well-being, should emphasize the risks of using fireplaces and heaters indoors, especially in bedrooms. In addition to the risks of inhaling particulate matter, the products of combustion and thermal degradation lead to the formation of substances that irritate the respiratory epithelium with a potential risk of exacerbating asthma.45
Fragrances and the Respiratory Tract
Although most of the substances used to generate the fragrance of perfumes are benign, a minority have the potential to cause adverse health effects, notably allergic contact dermatitis resulting from skin sensitization to compounds such as isoeugenol or eugenol. As a result, industry guidelines, as well as comprehensive trade bodies, of which perhaps the most important is International fragrance Association (IFRA), have banned certain materials and strictly limited the use of others in their products.46
In a recent review, Basketter et al concluded that mechanisms of allergic sensitization with the use of fragrances seem highly unlikely to occur in the respiratory epithelium. Although some sensory/psychosomatic effects are possible, adverse effects to the respiratory tract resulting from fragrance inhalation are uncommon and minimal, with low irritating characteristics, which highlight the need for methodologically rigorous studies supported by the Bradford Hill causality criteria, based on the biological plausibility of the reaction of the indicated substance. Preferably, guidelines for caregivers are related to the excess of these products in closed environments, which should be avoided, especially those containing strong fragrances.47
Volatile Pool Compounds
The need for entertainment space at home has become urgent in recent years, both due to the current behavior of society and the safety and comfort that are generated. The presence of a swimming pool in a residential environment or even its use in leisure environments are reasons for constant concern by caregivers of children who suffer from allergic respiratory processes.48
Regular physical activity in people with controlled asthma is recommended, as it improves general health and physical resistance, as well as improves parameters of cardiopulmonary capacity, although it is known that increased physical activity can cause exertional bronchial spasm and exacerbation of bronchial asthma in some partially controlled patients.49
During swimming, bronchial ventilation can increase by 20 to 30 times, which can lead to a change in breathing pattern from nasal to mixed (nasal and pulmonary). Hyperventilation and cold air can induce bronchial spasm through water loss and increased osmolarity in bronchial tissues which, in turn, trigger the release of cellular inflammatory mediators, histamine, prostaglandin, and leukotrienes. In addition, increased bronchial ventilation promotes the penetration of air pollutants, allergens and other nearby irritants. Despite this, swimming is associated with less intensity of post-exercise bronchial spasm compared to running or other sports with the same intensity.50
The most used method of disinfecting swimming pools is the addition of chlorine, however, the reactivity of chlorine to compounds present in the body of a swimmer, such as the epidermis, urine, sweat, remains of impurities, results in the formation of a wide range of disinfection by-products (DBPs) such as monochloramines, dichloramines, trichloramines, trihalogenomethanes, haloacetic acid, some of which are known to be associated with adverse effects on the respiratory epithelium. Among the DBPs formed in swimming pools, among which more than 10 volatile compounds can be found, is trichloramine (NCl3). NCl3 is formed as a by-product of disinfection in chlorinated pools and can be found in liquid and gaseous phases.51
In a Cochrane systematic review, the authors collected data from randomized clinical trials (RCTs) and quasi- RCTs of children and adolescents comparing swimming with other physical activity and concluded that there was no evidence that swimming caused adverse effects in asthma control in young people under 18 years of age with stable asthma of any severity. In a more recent meta-analysis, using RCTs, quasi-experimental studies and intervention studies with disinfection products for swimming pools, the authors concluded that swimming did not result in adverse effects, on the contrary, it resulted in a reduction in bronchial hyperreactivity and bronchospasm exercise-induced.52
Due to the growing publications on the risks of DBPs in the respiratory tract of home recreational swimmers, there is a need for comparative studies between pool chlorine and other disinfectants considered alternatives, such as ozone, ultraviolet radiation, bromine and salt, in addition to silver and copper ions. The most suitable microbiological and chemical method is the ozonation of water, however, due to the high cost, this method is little used. In the case of using pools with chlorinated water, the guidance to caregivers is that patients with controlled asthma should practice all sports, including swimming. It is important that the pool has air circulation and is installed in an open environment to facilitate the dispersion of compounds suspended in the air.53
Exposure of Pesticides at Home
Pesticides are identified as chemical products that can be presented in different formulations and concentrations to be used in different environments: family farming, domestic use, animal sanitary bath and vector control. Situations of exposure vulnerability to these products can be identified regarding: improper disposal of containers, storage in internal rooms of the house, inadequate agricultural practices and lack of awareness of the potential dangers of these products, promoting a greater risk of harmful effects on the environment health during childhood. The concern with children’s exposure to pesticides is related to their toxic properties and the special vulnerability to exposure, which can occur from the prenatal period to older ages.54
There is a wide variety of chemicals (more than 9000 globally), presented in different formulations and concentrations. The classification of pesticides can correspond to their assignment, for example, insecticides, herbicides, fungicides, disinfectants, repellents and rodenticides. Another practical approach is to classify according to recommendations for use, for example, products for gardening, vector control, veterinary (animal baths) and agricultural.26
In general, children constitute a special exposure group, which can occur through multiple routes (transplacental, inhalation, skin and ingestion) simultaneously or sequentially during life. Inhalation of toxic substances occurs through breathable particles or aerosols that are spread by direct application of the product at home or through residual volatile vapors from pesticides applied adjacent to the home.55
Rural households are in an even more dangerous scenario, because children can inhale pesticides that are sprayed on freshly treated crops in the home area or have these products stored indoors. Some pesticides are well known and are part of the products that can be inhaled, among them acaricides (carbamates, nitrophenol derivatives, organochlorine compounds, organophosphate compounds), fungicides (dinitrophenols, thiocarbamates and dithiocarbamates, sulfur), herbicides (anilides, sulfonylureas, paraquat), insecticides (carbofuran, malathion, cypermethrin), rodenticides (warfarin) and repellents (diethyltoluamide). All these pesticides have a common characteristic, when applied they become volatile and can trigger an intense irritative process in the respiratory epithelium, some even pulmonary fibrosis, such as paraquat.54,56
Health professionals who assist patients, who come mainly from rural areas, must be careful to take a good clinical history and identify the pesticides that can cause clinical worsening of asthma. Once factors that facilitate the child’s exposure to these products have been identified, their caregivers need to be instructed to avoid handling and using them at home. Alternatives to the use of natural products should be encouraged to replace these pesticides.56
Reflections on the Role of the Caregiver in Integration with Asthma Patient Health Maintenance
One of the main effective actions in asthma management is to avoid exposure to environmental allergens, pollutants and inhaled irritants. In the pediatric population, asthma reflects some singularities, since children and adolescents are passive agents and the greatest demand for maintaining adequate environmental control falls on caregivers.1
Although there is no description in the literature of publications on the caregiver’s sense of coherence and environmental control in asthma, this article presents a new look at an old problem, now guided by the salutogenic perspective: promoting a healthy home environment, with reduction and prevention of exposure to pollutants and inhaled irritants will have positive repercussions on the clinical control of asthma.
Previous studies have shown that a high sense of coherence is related to better health outcomes, and this has been observed in the care of diabetic patients, with neurological diseases, autoimmune diseases, neoplastic diseases, in oral health care and even during the covid-19 pandemic.57,58 SOC, a construct of Antonovsky ‘s salutogenic theory, is a personal orientation for identifying, coping and solving problems, which has become a fundamental concept in public health, particularly for health promotion.59
Antonovsky ‘s inspiration for researching this phenomenon came when he studied climacteric women who had lived in concentration camps during World War II, finding that some of them maintained good physical and mental health. For the creator of the salutogenic theory, SOC has a direct effect on people’s health status, acting in such a way as to stimulate behavior patterns that promote health benefits. The SOC would be related to the ability to perceive one’s own body and the environment that surrounds it, determining whether the situation to which the individual is exposed is dangerous, safe or pleasant.10
The formation of the SOC is a continuum, being developed in childhood, built through the interactions of the social and family environment, and formed around 30 years of life, and can be extended to more advanced ages. It is believed that the SOC is an individual resource that can influence health behaviors, in the search for better clinical control, especially of chronic diseases.11
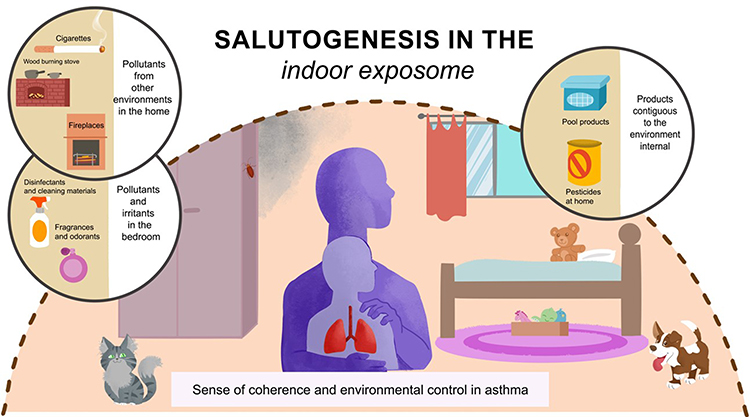
From the perspective of clinical asthma control, a high SOC may promote changes in the household exposure. Not only will aeroallergens be identified and avoided, but pollutants and inhaled irritants will be removed from the environment, especially from children and adolescents with asthma. Caregivers of patients with asthma will be the modifiers of the home environment, making the living space adequate to prevent asthma exacerbations. Figure 3 illustrates, in addition to environmental allergens, the main products and irritants that can affect the health of asthmatics and the role of protection and promotion of asthma control from the salutogenic perspective of a caregiver.12
 |
Figure 3 Home scenario with possible allergens, pollutants and harmful inhalation irritants for the child with asthma, highlighting the role of the caregiver, under the salutogenic perspective.
|
Conclusion
As part of the development of strategies regarding environmental control measures, a history of the home environment should be obtained to assess the main exposures to which the patient with asthma is subject. Environmental control approaches should be evidence-based and aimed at reducing these exposures as an important part of asthma management.1
Personalized and multifaceted environmental interventions, particularly in the home environment, are endorsed by international guidelines and may be similar in terms of effectiveness to controller medications. Environmental control measures for total removal of the source (eradication of the allergen or inhaled irritant), mitigation strategies (reduction of the amount of these substances in the air) and source control (control in the production of inhaled pollutants) have been described and advocated by the main guidelines of asthma, such as the National Asthma Education and Prevention Program (NAEPP) and the Global Initiative for Asthma (GINA).60
One of the limitations of current knowledge is that many other substances in the future may be identified as related to exacerbations and clinical worsening of asthma and have not yet been analyzed in studies with adequate methodology, as the topic is broadly addressed.
Environmental control recommendations, therefore, include prior knowledge of the most common pollutants and inhaled irritants that can be found at home; guidance and education for caregivers of children and adolescents with asthma on how to reduce exposure; adaptation of environmental control measures according to the patient’s socioeconomic conditions and the participation of public health policies in facing the commercialization of products that are known to be harmful to health, in particular to the respiratory epithelium.
Studies that investigate the relationship between the caregiver’s SOC and clinical control of asthma, focusing on home environmental control, are important and necessary, so that intervention measures can be effectively adopted for the adequate management of asthma in the pediatric population.
Abbreviations
ICSs, inhaled corticosteroids; IL, interleukin; Th, helper T; IgE, immunoglobulin E; TSLP, thymic stromal lymphopoietin; SOC, sense of coherence; PM, particulate matter; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; DBPs, disinfection byproducts; NCl3, trichloramines; EDTA, ethylenediamine tetraacetic acid; CFCs, chlorofluorocarbons; HCFC, hydrochlorofluorocarbon; IFRA, international Fragrance Association; RCTs, randomized clinical trials; NAEPP, national asthma education and prevention program; GINA, global initiative for asthma.
Acknowledgments
The authors would like to acknowledge the Postgraduate Program in Child and Adolescent Health linked to the Coordination for the Improvement of Higher Education Personnel (CAPES) and the National Council for Scientific and Technological Development (CNPq).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific funding.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Martin J, Townshend J, Brodlie M. Diagnosis and management of asthma in children. BMJ Paediatr Open. 2022;6(1):e001277. doi:10.1136/bmjpo-2021-001277
2. Hurst JH, Zhao C, Hostetler HP, Ghiasi Gorveh M, Lang JE, Goldstein BA. Environmental and clinical data utility in pediatric asthma exacerbation risk prediction models. BMC Med Inform Decis Mak. 2022;22(1):108. doi:10.1186/s12911-022-01847-0
3. Altman MC, Calatroni A, Ramratnam S, et al. Endotype of allergic asthma with airway obstruction in urban children. J Allergy Clin Immunol. 2021;148(5):1198–1209. doi:10.1016/j.jaci.2021.02.040
4. Papi A, Brightling C, Pedersen SE, Reddel HK. Asthma. Lancet. 2018;391(10122):783–800. doi:10.1016/S0140-6736(17)33311-1
5. Celebi Sozener Z, Ozdel Ozturk B, Cerci P, et al. Epithelial barrier hypothesis: effect of the external exposome on the microbiome and epithelial barriers in allergic disease. Allergy. 2022;77(5):1418–1449. doi:10.1111/all.15240
6. Cockcroft D. Environmental causes of asthma. Semin Respir Crit Care Med. 2018;39(01):012–018. doi:10.1055/s-0037-1606219
7. Rosário Filho NA, Urrutia-Pereira M, D’Amato G, et al. Air pollution and indoor settings. World Allergy Organ J. 2021;14(1):100499. doi:10.1016/j.waojou.2020.100499
8. Subramanian A, Khatri SB. The exposome and asthma. Clin Chest Med. 2019;40(1):107–123. doi:10.1016/j.ccm.2018.10.017
9. Busse WW, Kraft M. Current unmet needs and potential solutions to uncontrolled asthma. Eur Respir Rev. 2022;31(163):210176. doi:10.1183/16000617.0176-2021
10. d’Alessio PA. Salutogenesis and beyond. Dermatol Ther. 2019;32(1):e12783. doi:10.1111/dth.12783
11. Lindström B, Eriksson M. Contextualizing salutogenesis and antonovsky in public health development. Health Promot Int. 2006;21:238–244. doi:10.1093/heapro/dal016
12. Bhattacharya S, Pradhan KB, Bashar MA. Salutogenesis: a bona fide guide towards health preservation. J Fam Med Prim Care. 2017;6(2):169–170. doi:10.4103/jfmpc.jfmpc
13. Leas BF, D’Anci KE, Apter AJ, et al. Effectiveness of indoor allergen reduction in asthma management: a systematic review. J Allergy Clin Immunol. 2018;141(5):1854–1869. doi:10.1016/j.jaci.2018.02.001
14. Custovic A, de Moira AP, Murray CS, Simpson A. Environmental influences on childhood asthma: allergens. Pediatr Allergy Immunol. 2023;34(2):1–19. doi:10.1111/pai.13915
15. Raju S, Siddharthan T, McCormack MC. Indoor air pollution and respiratory health. Clin Chest Med. 2020;41(4):825–843. doi:10.1016/j.ccm.2020.08.014
16. Neophytou AM, Oh SS, White MJ, et al. Secondhand smoke exposure and asthma outcomes among African-American and Latino children with asthma. Thorax. 2018;73(11):1041–1048. doi:10.1136/thoraxjnl-2017-211383
17. Sugier P, Sarnowski C, Granell R, et al. Genome‐wide interaction study of early‐life smoking exposure on time‐to‐asthma onset in childhood. Clin Exp Allergy. 2019;49(10):1342–1351. doi:10.1111/cea.13476
18. He Z, Wu H, Zhang S, et al. The association between secondhand smoke and childhood asthma: a systematic review and meta‐analysis. Pediatr Pulmonol. 2020;55(10):2518–2531. doi:10.1002/ppul.24961
19. Niu X, Jones T, BéruBé K, Chuang HC, Sun J, Ho KF. The oxidative capacity of indoor source combustion derived particulate matter and resulting respiratory toxicity. Sci Total Environ. 2021;767:144391. doi:10.1016/j.scitotenv.2020.144391
20. Weinmann T, Forster F, von Mutius E, et al. Association between occupational exposure to disinfectants and asthma in young adults working in cleaning or health services. J Occup Environ Med. 2019;61(9):754–759. doi:10.1097/JOM.0000000000001655
21. Lindström I, Ryhänen A, Jungewelter S, Suojalehto H, Suuronen K. Asthma onset after exposure to fluorinated hydrocarbons in the presence of combustion. Am J Ind Med. 2020;63(11):1054–1058. doi:10.1002/ajim.23181
22. Saijo Y, Yoshioka E, Sato Y, et al. Relations of mold, stove, and fragrance products on childhood wheezing and asthma: a prospective cohort study from the Japan Environment and Children’s Study. Indoor Air. 2022;32(1):1–9. doi:10.1111/ina.12931
23. Kanikowska A, Napiórkowska-Baran K, Graczyk M, Kucharski M. Influence of chlorinated water on the development of allergic diseases – an overview. Ann Agric Environ Med. 2018;25(4):651–655. doi:10.26444/aaem/79810
24. Hwang SH, Park WM. Indoor air concentrations of carbon dioxide (CO2), nitrogen dioxide (NO2), and ozone (O3) in multiple healthcare facilities. Environ Geochem Health. 2020;42(5):1487–1496. doi:10.1007/s10653-019-00441-0
25. Lebel ED, Finnegan CJ, Ouyang Z, Jackson RB. Methane and NO x emissions from natural gas stoves, cooktops, and ovens in residential homes. Environ Sci Technol. 2022;56(4):2529–2539. doi:10.1021/acs.est.1c04707
26. Pascale A, Laborde A. Impact of pesticide exposure in childhood. Rev Environ Health. 2020;35(3):221–227. doi:10.1515/reveh-2020-0011
27. Butz AM, Tsoukleris M, Elizabeth Bollinger M, et al. Association between second hand smoke (SHS) exposure and caregiver stress in children with poorly controlled asthma. J Asthma. 2019;56(9):915–926. doi:10.1080/02770903.2018.1509989
28. Johansson E, Martin LJ, He H, et al. Second-hand smoke and NFE2L2 genotype interaction increases paediatric asthma risk and severity. Clin Exp Allergy. 2021;51(6):801–810. doi:10.1111/cea.13815
29. Merianos AL, Jandarov RA, Gordon JS, Lyons MS, Mahabee-Gittens EM. Child tobacco smoke exposure and healthcare resource utilization patterns. Pediatr Res. 2020;88(4):571–579. doi:10.1038/s41390-020-0997-0
30. Shen M, Li Y, Song B, Zhou C, Gong J, Zeng G. Smoked cigarette butts: unignorable source for environmental microplastic fibers. Sci Total Environ. 2021;791:148384. doi:10.1016/j.scitotenv.2021.148384
31. Clapp PW, Jaspers I. Electronic cigarettes: their constituents and potential links to asthma. Curr Allergy Asthma Rep. 2017;17(11):79. doi:10.1007/s11882-017-0747-5
32. Ratajczak A, Feleszko W, Smith DM, Goniewicz M. How close are we to definitively identifying the respiratory health effects of e-cigarettes? Expert Rev Respir Med. 2018;12(7):549–556. doi:10.1080/17476348.2018.1483724
33. Carson JL, Zhou L, Brighton L, et al. Temporal structure/function variation in cultured differentiated human nasal epithelium associated with acute single exposure to tobacco smoke or E-cigarette vapor. Inhal Toxicol. 2017;29(3):137–144. doi:10.1080/08958378.2017.1318985
34. Gakkhar A, Mehendale A, Mehendale S. Tobacco cessation intervention for young people. Cureus. 2022;14(10):1–7. doi:10.7759/cureus.30308
35. Liu C, Chen R, Sera F, et al. Ambient particulate air pollution and daily mortality in 652 cities. N Engl J Med. 2019;381(8):705–715. doi:10.1056/NEJMoa1817364
36. De Grove KC, Provoost S, Brusselle GG, Joos GF, Maes T. Insights in particulate matter-induced allergic airway inflammation: focus on the epithelium. Clin Exp Allergy. 2018;48(7):773–786. doi:10.1111/cea.13178
37. Ageel HK, Harrad S, Abdallah MAE. Occurrence, human exposure, and risk of microplastics in the indoor environment. Environ Sci Process Impacts. 2022;24(1):17–31. doi:10.1039/D1EM00301A
38. Hussain S, Parker S, Edwards K, et al. Effects of indoor particulate matter exposure on daily asthma control. Ann Allergy Asthma Immunol. 2019;123(4):375–380.e3. doi:10.1016/j.anai.2019.07.020
39. Wu J, Zhong T, Zhu Y, Ge D, Lin X, Li Q. Effects of particulate matter (PM) on childhood asthma exacerbation and control in Xiamen, China. BMC Pediatr. 2019;19(1):194. doi:10.1186/s12887-019-1530-7
40. Hadrup N, Frederiksen M, Wedebye EB, et al. Asthma‐inducing potential of 28 substances in spray cleaning products—assessed by quantitative structure activity relationship (QSAR) testing and literature review. J Appl Toxicol. 2022;42(1):130–153. doi:10.1002/jat.4215
41. Vizcaya D, Mirabelli MC, Gimeno D, et al. Cleaning products and short-term respiratory effects among female cleaners with asthma. Occup Environ Med. 2015;72(11):757–763. doi:10.1136/oemed-2013-102046
42. Clausen PA, Frederiksen M, Sejbæk CS, et al. Chemicals inhaled from spray cleaning and disinfection products and their respiratory effects. A comprehensive review. Int J Hyg Environ Health. 2020;229:113592. doi:10.1016/j.ijheh.2020.113592
43. Abrams EM. Cleaning products and asthma risk: a potentially important public health concern. Can Med Assoc J. 2020;192(7):E164–E165. doi:10.1503/cmaj.200025
44. Lawal AT. Polycyclic aromatic hydrocarbons. A review. Fantke P, ed. Cogent Environ Sci. 2017;3(1):1339841. doi:10.1080/23311843.2017.1339841
45. Lee YJ, Jeong IB. Chemical pneumonitis by prolonged hydrogen fluoride inhalation. Respir Med Case Rep. 2021;32:101338. doi:10.1016/j.rmcr.2020.101338
46. Santana FPR, da Silva RC, Ponci V, et al. Dehydrodieugenol improved lung inflammation in an asthma model by inhibiting the STAT3/SOCS3 and MAPK pathways. Biochem Pharmacol. 2020;180(May):114175. doi:10.1016/j.bcp.2020.114175
47. Basketter DA, Huggard J, Kimber I. Fragrance inhalation and adverse health effects: the question of causation. Regul Toxicol Pharmacol. 2019;104(March):151–156. doi:10.1016/j.yrtph.2019.03.011
48. Andersson M, Backman H, Nordberg G, et al. Early life swimming pool exposure and asthma onset in children – a case-control study. Environ Heal. 2018;17(1):34. doi:10.1186/s12940-018-0383-0
49. Beggs S, Foong YC, Le HCT, Noor D, Wood-Baker R, Walters JAE. Swimming training for asthma in children and adolescents aged 18 years and under. Cochrane Database Syst Rev. 2013;2013(4). doi:10.1002/14651858.CD009607.pub2
50. Seys SF, Feyen L, Keirsbilck S, Adams E, Dupont LJ, Nemery B. An outbreak of swimming-pool related respiratory symptoms: an elusive source of trichloramine in a municipal indoor swimming pool. Int J Hyg Environ Health. 2015;218(4):386–391. doi:10.1016/j.ijheh.2015.03.001
51. Wu T, Földes T, Lee LT, et al. Real-time measurements of gas-phase trichloramine (NCl 3) in an indoor aquatic center. Environ Sci Technol. 2021;55(12):8097–8107. doi:10.1021/acs.est.0c07413
52. Ramachandran HJ, Jiang Y, Shan CH, Tam WWS, Wang W. A systematic review and meta-analysis on the effectiveness of swimming on lung function and asthma control in children with asthma. Int J Nurs Stud. 2021;120:103953. doi:10.1016/j.ijnurstu.2021.103953
53. Päivinen M, Keskinen K, Putus T, Kujala UM, Kalliokoski P, Tikkanen HO. Asthma, allergies and respiratory symptoms in different activity groups of swimmers exercising in swimming halls. BMC Sports Sci Med Rehabil. 2021;13(1):119. doi:10.1186/s13102-021-00349-2
54. Rodrigues MDB, Carvalho DSD, Chong-Silva DC. Association between exposure to pesticides and allergic diseases in children and adolescents: a systematic review with meta-analysis. J Pediatr. 2022;98(6):551–564. doi:10.1016/j.jped.2021.10.007
55. Islam JY, Hoppin J, Mora AM, et al. Respiratory and allergic outcomes among 5-year-old children exposed to pesticides. Thorax. 2023;78(1):41–49. doi:10.1136/thoraxjnl-2021-218068
56. Fishwick D, Harding AH, Chen Y, Pearce N, Frost G. Asthma in pesticide users: an update from the Great Britain Prospective Investigation of Pesticide Applicators’ Health (PIPAH) cohort study. Occup Environ Med. 2022;79(6):380–387. doi:10.1136/oemed-2021-107486
57. Polhuis KCMM, Vaandrager L, Koelen MA, Geleijnse JM, Soedamah-Muthu SS. Effects of a salutogenic healthy eating program in type 2 diabetes (the SALUD Study): protocol for a randomized controlled trial. JMIR Res Protoc. 2023;12:e40490. doi:10.2196/40490
58. Tóth ÁL, Kívés Z, Szovák E, et al. Sense of coherence and self-rated aggression of adolescents during the first wave of the COVID-19 pandemic, with a focus on the effects of animal assisted activities. Int J Environ Res Public Health. 2022;20(1):769. doi:10.3390/ijerph20010769
59. Drageset S, Ellingsen S, Haugan G. Salutogenic nursing home care: antonovsky’s salutogenic health theory as a guide to wellbeing. Health Promot Int. 2023;38(2):1–11. doi:10.1093/heapro/daad017
60. Kader R, Kennedy K, Portnoy JM. Indoor environmental interventions and their effect on asthma outcomes. Curr Allergy Asthma Rep. 2018;18(3):17. doi:10.1007/s11882-018-0774-x








![2023-2031] Computer and Gaming Glasses Market Current Trends and Growth Opportunities](https://media.licdn.com/dms/image/D4D12AQFnRKwwXER2vA/article-cover_image-shrink_600_2000/0/1696480458135?e=2147483647&v=beta&t=JCE4eq7kfa-S5sgEsYiO0anP0HVUetqj3hMOUz3dh94)



















