One of the two first responders responsible for the death of the young African-American Elijah McClain in 2019 was sentenced to 14 months in half-term detention on Friday. McClain died after his arrest when emergency workers injected ketamine to calm him down.
The paramedic will still be allowed to work during the day, but must return to prison in the evenings and on weekends during his sentence, a Colorado court ruled. In addition, he was given a four-year suspended prison sentence. Paramedic Jeremy Cooper and his colleague were found guilty of involuntary manslaughter in December.
Elijah McClain was put in a chokehold during his arrest in the city of Aurora and was subsequently injected with the strong sedative. The 23-year-old died three days later of a heart attack. The case only gained media attention after the death of George Floyd, another young American with black skin, in May 2020.
During the trial, the first responders stated that they were only following procedures when they administered the ketamine. The public prosecutor’s office refuted this and accused them of not having talked to the victim and that they had not checked his heart rate and breathing before administration.
In January, one of the three police officers involved was sentenced to 14 months in prison. At another trial, the two others were acquitted.
McClain was stopped by police on the street after an anonymous caller said he looked “mysterious” – he was wearing ski goggles. According to the victim’s family, he was outside to buy an ice tea. According to them, he often wore a ski buttock to avoid getting cold, as he suffered from anemia.
The use of ketamine in arrests is controversial in the US. Investigations have already been launched in several states.
The former
world No. 1 Kim Clijsters commented on a panic attack she experienced in the
2021 Indian Wells. The Belgian returned to tennis for the second time in 2020
after 7 years since her retirement and played two tournaments in the Dubai Open
and Monterrey Open, but her comeback was halted when the Covid-19 pandemic
forced the cancellation of tournaments between March and July of that year.
After the
pandemic, she barely played a couple of matches before contracting COVID-19,
which once again kept her off the courts. In October 2021, Clijsters
participated in Indian Wells, which was postponed from March to October, and
was eliminated in the first round against Katerina Siniakova.
The 4-times
Grand Slam champion was invited to the program "Served with Andy
Roddick" and commented that she experienced a panic attack for the first
time while preparing to participate in Indian Wells.
"I
remember hitting with Kiki Bertens and Ajla Tomljanovic and I had such good
practices, be it practice sets, be it beating girls in practice, but I just
wanted to kind of prove it in a match,” the former world No. 1 started.
“And during
one of the practices I just started like, yeah, really I had a panic attack on
the tennis court. For a second, I felt like I was being a drama queen,"
Clijsters added.
"My
trainer was like 'Just lay down, put your legs up', and that, like, me calming
down, or that wasn't working at all. So I was like, to my tennis coach, 'Go
stand at the net and hit towards me'. So I had the rhythm and the sound of the
ball, and my breathing rhythm came back," she concluded.
Respiratory ailments never bothered my husband, Randy, or me in Fort Worth, Texas, where we grew up. Columbia, South Carolina, our destination in 1985, was wretchedly muggy but didn’t prompt any allergy issues, either.
In the early 1990s, we moved to Lenoir, North Carolina, where furniture factories thrived. That would’ve been fine had our son, Matthew, not attended an elementary school smack-dab in the middle of prolific pollution. His allergy symptoms gradually worsened over the next few years until one night, his breathing struggles landed us in the emergency room for an asthma diagnosis. An inhaler was prescribed.
Asthma was quite prevalent in Lenoir, so sure enough, not long after our daughter, Katie, entered kindergarten at the same school, she snagged an inhaler of her own.
In the middle of the following school year, with Matthew in fourth grade and Katie in first, we moved to the North Carolina mountains. The myriad adjustments kept life lively: a blizzard, flying squirrels in the house, salamanders in our drinking water, and a single bathroom with a temperamental toilet, for starters.
It didn’t take long to recognize the most exciting revelation: The clear air in our new rural area apparently rendered inhalers unnecessary. I was elated that respiratory issues were history!
But I was wrong.
Recommended Reading
SMA’s destructive nature
Our third baby, Jeffrey, delivered a few surprises to us, starting with the positive pregnancy test. His arrival on May 18, 1997, came two weeks ahead of schedule. He was such an exceptionally contented, quiet baby that I jokingly wondered if we’d be making up for it during his teen years.
We didn’t get the opportunity to find out. A diagnosis of spinal muscular atrophy (SMA) gobsmacked us eight weeks after Jeffrey’s arrival. Life for the next three and a half months was spent in survival mode, both for him and for us.
Baby Jeffrey Baldwin in 1997. (Photo by Helen Baldwin)
Although SMA packs a potent punch, it was the respiratory struggles that left me limp. Seared into my memory are images of the panic in Jeffrey’s eyes during an impromptu, ill-fated In-Exsufflator trial and as SMA’s progression wreaked unforgiving havoc on his ability to breathe.
Jeffrey wrangled free from SMA’s deadly clutches before he reached six months. Witnessing your child’s final breath is devastatingly surreal. It isn’t normal in the scheme of things. However, neither is pumping your baby full of morphine, suctioning secretions every few minutes, and praying for God to take him.
As we adjusted to the unthinkable, our heavy hearts relied on reminders that Jeffrey was in the perfect place, safe from harm.
Incredibly, our family remained fairly and uneventfully upright for years.
Gasping for air
Years after our SMA assignment ended, I awoke one morning gasping for air. It was promptly deemed an emergency. I was treated in a hospital emergency room for reactive airway disease and given several prescriptions, including a pearl that would paralyze my throat if I bit down on it. I didn’t.
Since the ER folks couldn’t tell what had happened, I racked my brain until I hit upon a plausible culprit. Our old farmhouse doesn’t have air conditioning, so unless there’s a monsoon, the windows generally remain open from spring until fall. My computer is situated in front of a tall window on the side of the house mere yards from a small creek. The property on the other side of the creek tends to be untamed, as they say.
During a particularly chaotic schedule, Randy and I had hired someone to mow and cut weeds. It happened to be unusually dry at the time. Because our yard person mowed and used a Weed Eater with abandon, it was likely that the dry stuff being churned up and spit out in the direction of my window — and my lungs — included poison ivy, poison oak, and other irritants. It made sense that I’d likely breathed dust from pulverized poison ivy — an unfortunate event because now I know what to do next time.
Thankfully, next time didn’t come, and breathing issues became a moot point.
And then came James.
Battling different breathing challenges
Our grandson, James Baldwin, in 2018. (Photo by Helen Baldwin)
Randy and I are PopPop and MomMom to two delightful grandchildren, Clara and James. Clara’s diagnosis of Beckwith-Wiedemann syndrome caught us off guard. Her case is mild, and we breathed a sigh of relief when it seemed a certainty that James wouldn’t follow suit.
At 14 months, though, James experienced such a horrific case of croup that he was admitted to a local hospital. Within hours of dismissal, he was on his way to a more sophisticated hospital for additional treatment. Seeing Matthew and our daughter-in-law, Jill, being utterly exhausted while driving off with a very sick little James unleashed a few memories, especially since their destination was Brenner Children’s Hospital in Winston-Salem, North Carolina, where Jeffrey was diagnosed.
Today, James, 6, still experiences occasional respiratory issues that are significant. The doctor expects him to outgrow them, but until then, I’m confident that his angel “twin” will be breathing right along with him.
Because he can.
Note: SMA News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. The opinions expressed in this column are not those of SMA News Today or its parent company, BioNews, and are intended to spark discussion about issues pertaining to spinal muscular atrophy.
When a young mother complained to paramedics she was suffering chest pains, cold sweats and her lips were going black, she was told to take Panadol and follow up with a GP.
Within 48 hours, she was dead.
On Wednesday, a South Australian coroner found Jennifer Collins, 30, would likely still be alive if not for a series of missteps by those overseeing her treatment.
Deputy State Coroner Ian White said vital information was not passed on from paramedics to hospital staff, doctors missed a blood test that could have prevented her misdiagnosis and a heart rate reading was incorrectly transcribed at a crucial juncture in her care.
"In light of the findings made above, I find Ms Collins' death was preventable," he said in his report.
Ms Collins died on September 6, 2018, leaving a six-year-old son.
She was "very empathetic and kind", but had struggled through her life with childhood trauma, abuse and drug addiction, her doting brother Bryon told the coroner.
Her cause of death was determined as infective endocarditis; a rare inflammation of the heart's lining, but which is more prevalent in intravenous drug users.
Shortly before her death, Ms Collins was attempting to kick a crippling meth addiction - a critical factor in the misdiagnosis of her condition and the decision-making of medical staff.
She first called triple zero on August 20, describing herself as having a heart attack with tightness in her chest and difficulty breathing.
However, due to her tight financial circumstances, she elected not to go to Port Noarlunga Hospital via ambulance and was instead driven there by her stepfather.
This resulted in a disconnect in communication, as paramedics were not able to advocate her condition to hospital staff, Mr White found.
The hospital subsequently decided not to investigate her condition using a blood culture test, a "pivotal decision", according to the coroner.
"I find that if this had been done then, her death was likely to have been prevented as infective endocarditis would have been identified," he said.
Instead, the possibility of Ms Collins having infective endocarditis was "inappropriately discounted" and the incorrect decision to discharge her was made.
On September 4, her brother Bryon made another emergency call to SA Ambulance Service, reporting she was suffering major chest pain, was breathing rapidly, had a yellow complexion, and her lips were going black.
Shaun Falls, an experienced and "extremely competent" paramedic, attended her home and tested her vital signs.
He found them all to be within acceptable ranges, except for Ms Collins' heart rate which was slightly elevated, so advised against going to hospital and told her to follow up with a GP.
However, in manually transcribing Ms Collins' readings, he incorrectly recorded her pulse as 110 bpm and 112 bpm, instead of 136 bpm and 137 bpm, which should have raised a red flag.
Mr White said the paramedic may have downgraded Ms Collins' priority assessment and cancelled ambulance transport too hastily.
"I am concerned that Mr Falls may have either consciously or subconsciously assessed her as a drug user seeking to withdraw from her habit and that her body was suffering the physical consequences," the coroner said.
Ms Collins died two days later.
Mr White recommended medical staff be better educated on the diagnosis of infective endocarditis and the higher risk experienced by drug users.
He also urged a review into information-sharing between SA hospitals and the ambulance service.
Audie Liametz, Vice Chairman of the Emergency Department at NYU Langone Hospital, explains how diving into cool water could put you at risk in the summer.
We can get hypothermia in the air when the temperature is 60 degrees, but cold water saps the body of heat much faster.
Hypothermia can happen in water as warm as 80 degrees, while water that is 64 degrees could be deadly, according to the University of Michigan.
"Immersion in cold water can become life-threatening very quickly," wrote the NWS office in Burlington, Vermont. "Since water conducts body heat away up to 25 times faster than air of the same temperature, the cold water rapidly causes extremities to become numb, weakens the ability of muscles to work effectively and eventually leads to hypothermia."
File: Even swimmers that have cold water training must exit the lake in this Vermont Festival swim meet after 5 minutes.
(Jessica Rinaldi / The Boston Globe / Getty Images)
It doesn't necessarily mean that just people falling through ice are in danger. Even during a heatwave, water temperatures can be chilly.
Cold shock
The first danger of cool water is "cold shock."
Cold shock can be just as severe and dangerous from water temperatures of 50-60 degrees as it is from water at 35, according to the NWS.
Gasping for a breath or rapid breathing from sudden immersion can be triggered by water as warm as 77, according to the NWS.
"When your body hits cold water, ‘cold shock’ can cause dramatic changes in breathing, heart rate and blood pressure," wrote NOAA. "The sudden gasp and rapid breathing alone creates a greater risk of drowning even for confident swimmers in calm waters. In rougher open water, this danger increases."
File: Colorado crews practicing cold water rescues when minutes matter.
(Evergreen Fire and Rescue / FOX Weather)
Cold shock can cause panic, which impairs clear thinking and decision-making. It can also cause a sudden spike in heart rate and blood pressure, which can lead to a heart attack or stroke. Severe pain from the cold also clouds thinking.
While cold shock diminishes after the first 1-3 minutes of sudden immersion, the body continues to lose heat. Even a person who has been pulled out of the water can still lose body heat. Wet clothes increase the body's heat loss by five times over the general 2% of body heat lost to the environment. Hypothermia, the body dropping to or below 95 degrees, comes in stages and degrees.
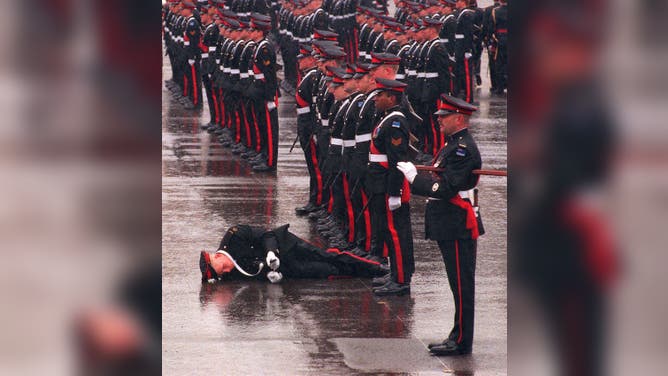
File: A cadet at the Royal Military College Duntroon in Australia succumbs to hypothermia in freezing temperatures and a wet uniform.
(NEWS LTD/AFP / Getty Images)
"So initially, you are in the water, and you start getting cold, and you start shivering, maybe develop slurred speech. You have some confusion, pulse may get a little weak," Audie Liametz, Vice Chariman of the NYU Lagone Hospital Emergency Department, told FOX Weather over the summer. "And then it can progress from mild hypothermia to moderate hypothermia, where you start having alteration in the mental status."
Coordinated hand and finger movements can cease within minutes, which makes grabbing the edge of the water or a float for self-rescue difficult, according to the University of Minnesota Sea Grant, a water safety program.
"Swimming or treading water will greatly increase heat loss and can shorten survival time by more than 50%," warned USSARTF.
Hypothermia often occurs at very cold temperatures, but you can still be susceptible at temperatures as warm as 60 degrees.
As hypothermia progresses, it strips the body of its automatic responses to combating cold.
"When it gets to very severe hypothermia, you can actually lose the shivering response," Liametz said. "Because the shivering response is the body's reaction to keeping the temperature warm. It warms you up by contracting the muscles," Liametz continued.
The normal body temperature is 98.6 degrees. Shivering starts at 96.5. Amnesia can start at 94. Brain function declines when the body temperature is 91 degrees, with unconsciousness at 86 degrees. The heart and breathing slow at 84 degrees. The human heart can stop at 64 degrees, according to Sea Grant. USSARTF stated that death can happen when the body is 79 degrees.
Flotation devices can prevent drowning even if a person is unable to swim, allowing more time for rescue. A person can become incapacitated or unconscious in cold water in as little as 9 minutes without a life jacket. With a life jacket, that time rises to 15 minutes.
Mar. 26—There are about 37 million adults in the U.S. that are living with chronic kidney issues, but about 90 percent don't know it.
You don't usually see symptoms, said Dr. Ike Okwuwa, program director and associate professor of Family and Community Medicine at Texas Tech University Health Sciences Center. Kidneys filter your blood, remove waste, balance water and nutrients and release some hormones to help regulate blood pressure, produce red blood cells and help with bone health.
"It's not just a filter. It does a lot of things," Okwuwa said of kidneys.
"It's a very, very important organ that I think it's our duty to try to protect," he added.
According to the Mayo Clinic website, "Signs and symptoms of kidney disease are often nonspecific. This means they can also be caused by other illnesses. Because your kidneys are able to make up for lost function, you might not develop signs and symptoms until irreversible damage has occurred."
Fatigue, anemia, protein in the urine which can make it foamy and swollen legs are signs of the disease, Okwuwa said. But by that time, the disease has progressed "a little bit more."
"A ton of people have CKD or chronic kidney disease and don't know about it ... It's very easy to test these things in the blood. Every year you go see your doctor. They can do a blood test for you. It shows how much your kidneys are still filtering, so the function of your kidneys. They can even do a urine test. That would show if your kidneys are ... leaking proteins," Okwuwa said.
He added that the two most common causes of chronic kidney issues in the United States are diabetes and high blood pressure. Obesity can also be a risk factor. It's recommended that people exercise 150 minutes a week, or about 30 minutes a day five days a week.
Controlling your high blood pressure, diabetes, salt intake, watching your diet, eating plenty of fruits and vegetables, quit smoking and staying hydrated and asking your doctor about any medications you might be taking that could impact your kidneys also helps.
Sometimes doctors may need to reduce the dose of some medications.
"It's going to have to be that good relationship between your doctor and (yourself) and watching," Okwuwa said.
If your primary care doctor thinks you need to see a nephrologist (a kidney doctor), they can refer you.
Should the disease progress too far, it's dialysis or a kidney transplant.
Kidney function is going to decline with age, starting at about age 60, he said. If you have a family history of kidney disease, it puts you more at risk.
If the kidneys are damaged, it increases the risk of heart attack and stroke. It also affects bone health.
The summer of 2020 shouldn’t project beautiful memories onto the brain maps of those who endured it, but Theda Hammel’s anxiety-addled screwball feature debut “Stress Positions,” set around that COVID Fourth of July in New York, asks you to relive the scary days of sheltering in place, banging pots and pans in solidarity with health care workers, and social distancing whenever it was convenient or made you look like you stood for something.
“Stress Positions” mines the gap between the dark bookend of events that shaped millennial lives — September 11 and the pandemic — and that between liberal-posturing millennials and a Gen Z with a less fussy, more hopeful worldview. Hammel’s muses and emissaries on either side of the dichotomy in a comedy swirling with ideas are comedian John Early as a gay soon-to-be-divorcee and Qaher Harhash as his nephew, a 19-year-old Moroccan model with identity-shifting questions of his own. Here is a movie that sees a hapless set of self-obsessed millennials who came of age out of liberal arts colleges and the internet for who they really are.
More from IndieWire
This caustic Brooklyn-set ensemble comedy awash in discourses around gender, social justice, and American ignorance of the Middle East is an energetic interrogation of what that kind of film — in other words, stuff that’s often very much the province of a Sundance indie — looks like in 2023. Early’s Terry Goon is a once-idealist turned politically indifferent basket case splitting up with his husband Leo (John Roberts), who’s left his shambling Brooklyn brownstone in Terry’s care while Leo runs off to Berlin in search of ketamine and other trade. (A great line later sees one character describe Fire Island, where Terry and Leo got married, as “a beach retreat for the children of Sodom.”) Trans filmmaker/writer Hammel casts herself as Carla, an ambitionless bodyworker in a foundering relationship with a lesbian named Vanessa Ravel (Amy Zimmer), whom Carla has accused of stealing her life story of transition as fodder for Vanessa’s debut novel. But it’s Carla who now enjoys the spoils of that book’s success, living rent-free in Vanessa’s apartment.
The 19-year-old and very beautiful Bahlul (Harhash) is Terry’s nephew, now convalescing with a broken leg in a brownstone whose own layout becomes as stress-inducing to navigate for the characters as it does the audience. Bahlul is the only son of Terry’s sister Abigail, shown only onscreen in fragmented home videos who, after fleeing the U.S. decades ago, converted to Islam, and returned to the U.S. with hate in her heart toward the Western world. The film’s slippery, though at times frustratingly overexpository, narration slides from Carla’s own to Bahlul’s as he explains his complicated family history.
“Stress Positions” packs a crazy gaggle of characters into a tight 90 minutes, expanding the film’s entropic little universe in providing three dimensions to nearly all introduced, everyone bouncing like speedy atoms off each other, including Grubhub courier Ronald (Faheem Ali, who shares a story credit with Hammel), who Carla seduces. The film’s commentary on immigrants forced to submit themselves to the gig economy is only skin-deep, but “Stress Positions” mostly succeeds in chewing off so much that any and all digressions from its core characters could risk shaking the focus too much.
Everyone but Bahlul — far more unflappable than his minders, and he doesn’t judge when everyone continues to make the mistake of misidentifying Morocco as a Middle Eastern country — is on the precipice of falling utterly apart. Carla, as so many of us did in the deep dog days of the pandemic, has taken to day-drinking to numb her boredom when not meddling with others’ lives or participating vaguely in protest (“we’re occupying,” she tells Terry when entreating him to join her at city hall, but for what the film never says though we can assume it’s related to the murder of George Floyd given the particulars of this COVID period piece).
When Bahlul asks her why she transitioned, Carla, in a hilarious and increasingly slurry grappa-soaked monologue, says, “I wanted to kill myself, and this helped,” a painfully funny line that rings with the real misery of uncertain identity in a wishy-washy world. Editor Erin DeWitt and cinematographer Arlene Muller create an atmosphere that never stops to breathe between panic attacks, especially as “Stress Positions” starts to feel like one big long one in desperate need of a Xanax or at least a session of four-quadrant breathing.
“Stress Positions” leaves unturned no hollow stone of millennial ideologies that now border on self-parody when stacked up against the category-eschewing sensibilities of the younger Generation Z, who here make a fool out of their forbearers. Vanessa is aggressively vegan, which is seemingly all she stands for, while Carla and Terry have a lot of thoughts about the “Arab world” but can’t name who actually orchestrated 9/11 and where Kabul is situated on a map. Bahlul does not make his politics the definition of his identity, a gesture seemingly the province of his millennial elders, and look how that turned out? They’re too caught up in their own neuroses and narcissistic bullshit to be politically committed to anything genuinely. Eventually, Bahlul becomes the heart of “Stress Positions,” as he forms a sweet connection with a chain-smoking upstairs neighbor (Rebecca F. Wright) with a voyeuristic agenda of her own.
Hammel and Early make for a wickedly funny pair, playing off each other’s misanthropy and deftly personifying what a long-term friendship that started a decade before in college now looks like in the 30s: “Not everyone is trans!” Terry screams at Carla, in a moment that feels designed to rile up corners of the audience (certainly not the target viewership here, and unlikely to see this film anyway) who will roll their eyes at the fact that literally every character in “Stress Positions” is queer in some way, something Hammel’s sharp script both celebrates and critiques.
John Early, first through his TV work as a quippy pop culturally literate New York gay in “Search Party” and his self-effacing standup, now again proves that he may truly be the voice of his generation (at least the cis white gay ones in the room). Here, he makes his body as much an instrument as his wit, literally flailing as his life crumbles around him, frantically applying Purell, Lysoling his groceries, wearing a garish respirator in the company of all around him. Terry is running in place — quite literally so on an exercise bike, sweatily, in the basement each night — but Early makes his existential inertia always feel like it’s compellingly headed some place, and that is a doomy kind of catharsis.
You wouldn’t be wrong to feel like at turns “Stress Positions” lays it on thick with social commentary and even overwhelms the audience with talky mouthpieces who all represent the far-flung quadrants of the issues at hand, whether immigration, globalization, sexuality, race, or lazy liberalism. But in its wryly amusing self-awareness at all turns, the film actively and relentlessly lampoons the very language and gesturing we all affect in trying to broach the political maelstrom of identity politics.
But all along, the film is carefully layering its cracked cast and meandering anecdotes toward a profoundly satisfying conclusion, even if “Stress Positions” feels like it leaves us and its characters hanging in the middle of its own unfinished sentence. There’s a Chekhov’s massage gun throughout the film — how applied in vain it is by the characters onto themselves as their only balm for relief from their own physically realizing anxieties — that brings the events cascading toward a chaotic climax where everyone’s positions are brought out into the light for what they are: phoneys, but real phoneys, and always headed for self-made disaster anyway.
Grade: B+
“Stress Positions” premiered at the 2024 Sundance Film Festival. Neon will distribute the film in the U.S. later this year.
Mistrust in legacy media is only growing, and when journalists publish articles that gaslight and invalidate millions of women's experiences, it's not hard to understand why. The Washington Post's recent article "Women are getting off birth control amid misinformation explosion" drew so much backlash on Instagram that they turned off the comments. Women's health professionals all over the internet critiqued the gaslighting attitude of the article.
Even the women interviewed for the article were not happy with how their personal experiences and knowledge of hormonal birth control were treated by The Washington Post. Many have shared their side of the story on social media or with Evie Magazine or both.
Sabrina Grimaldi, the founder of online magazine The Zillennial Zine, described to The Washington Post how her birth control gave her blood clots in both lungs and her leg. The newspaper mentioned her experience in brief (you can read her full story here on Evie) as an example of a rare side effect and skimmed over how, throughout Sabrina's whole experience, her questions and concerns were dismissed or ignored by each doctor she encountered. In a response on her Instagram, Sabrina said the article failed to fully connect the medical gaslighting to why women are turning to alternative sources for information about birth control.
Another interviewee, certified holistic nutritionist Nicole Bendayan, describes her interview with The Washington Post as "one of the most disingenuous experiences I've ever had" and took to social media to share her side of the story. Nicole says the article "falsely represented and tried to discredit me." She highlights that birth control and women's health are not political issues – they're health issues. She was "made to believe this would be a positive piece about how women are moving toward holistic health practices and away from hormonal birth control." Not only did The Washington Post turn her into a "pawn" for their political agenda, but they invalidated her own personal lived experience on birth control. Furthermore, The Washington Post positioned Nicole as an influencer and educator, conveniently leaving out her nutrition coaching certifications, which she says they were aware of.
The Washington Post also reached out to cultural commentator Alex Clark, the host of POPlitics and The Spillover Podcast, about hormonal birth control but failed to include her responses in their article. At Alex's request, we have included her answers below:
Washington Post: You have called birth control “poisonous” – can you explain why? What makes it poisonous?
Alex Clark: When something increases the risk of depression by 130% – that’s poison. When something may double your risk of breast cancer – that’s poison. When something increases your risk of blood clots by three-fold – and largely goes away within a couple of weeks if you stop taking it – that sounds an awful lot like poison. A substance that alters your personality so much that you choose a different romantic partner than you would when you’re not on it? That’s poison. Poison is defined as something that can cause illness or death. Hormonal birth control fits that standard.
WaPo: Why is there a movement among prominent conservative commentators, including yourself, to question the safety of hormonal birth control?
AC: The anti-birth control movement is not conservative, historically or currently. It started in the 1970s with a group of feminist, liberal women who spoke up and risked their reputations questioning Big Pharma at the Nelson Pill hearings. They demanded to know why women were being experimented on like guinea pigs, because we were seeing alarming health risks after 20 years of being prescribed the pill. In fact, it’s because of these liberal women that we are given an insert packet larger than a newspaper with birth control risks and side effects. The attack on women who happen to be conservative who are speaking out against the harms of birth control is disrespecting the very feminists they claim to admire. It was their backbreaking work to warn women around the world about the potential negative health consequences of birth control that planted the seeds for today’s pushback, a movement that is growing. This isn’t a partisan issue. This is a health issue that affects all women, regardless of political persuasion. Women from all political parties, religions, and regions should care that we have been encouraged to ingest a pill without an honest understanding of the hundreds of very real potential risks associated with it.
WaPo: Some experts say you are working to vilify hormonal birth control in order to limit access to it – do you have a response?
AC: “Some experts say.” Who are the experts? Who do they work for? Here’s what I am working toward: informed consent for women. No one is trying to ban anything. To suggest we are is a 2024 agenda to scare women. What we want is for young women to be fully educated about the potentially negative and harmful side effects so they can make the best, most informed decisions for their own health care. Ten minutes in a wellness checkup is not enough time for a doctor to explain the risks of taking this pill honestly and thoroughly to a 15-year-old girl struggling with acne. We have women being prescribed this medication as a band-aid cure-all to myriad other underlying health issues, from illnesses that could lead to infertility if untreated to serious hormonal disorders that require root-cause treatment. I’ve heard of countless stories of women who have described their experience of the pill masking deeper health issues they then were forced to deal with 10-15 years later when they are finally ready to have a baby. Sadly, many were unable to ever get pregnant because they failed to deal with underlying health issues years before trying to start a family. I don’t want that for the next generation.
And lastly, Evie Magazine's Editor-in-Chief Brittany Martinez was also among those interviewed by The Washington Post. She has written a full response to the paper, which you can read here.
Evie deserves to be heard. Support our cause and help women reclaim their femininity by subscribing today.
SINGAPORE – Shipyard engineer Jaime Mendoza, 57, suffered a stroke in September 2020.
The stroke affected his brain and his ability to breathe, so Mr Mendoza was given a tracheostomy, where a tube is inserted into his windpipe to allow air into his lungs. He was kept in the intensive care unit (ICU) for about a month before he was moved to the general ward.
The family had been out celebrating his daughter’s birthday when he suddenly felt unwell and was hurried by taxi to the emergency department of Tan Tock Seng Hospital (TTSH).
“He was in (the) hospital for the next three months. He came home for a month before being hospitalised at the Ang Mo Kio Rehabilitation Centre from March till May 2021,” his wife, Mrs Edna Mendoza, 57, told The Straits Times.
His seven-month stay, first at TTSH and then at the rehabilitation centre, would have been cut by close to three months – or an average of 81 days for such patients – if he had been taken directly from the ICU to the Ventilatory Rehabilitation Unit (VRU).
Patients with conditions and injuries that affect breathing, such as head injury, stroke, lung diseases, heart attack, pneumonia and spinal cord injuries, would do better when they are moved directly from the ICU to a specialised rehabilitation unit once their underlying conditions are stable, said Dr Lui Wen Li, a consultant with the Department of Rehabilitation Medicine at TTSH.
“In 2019, the average stay in hospital for patients needing ventilators to breathe was more than 200 days. We realised that rehabilitation is not the main focus of acute (care) hospitals.
“They cater more to managing the acute medical and surgical issues rather than specialised rehabilitation. Often, patients are not able to work towards improvement in speech, mobility and swallowing,” she said.
In 2020, the rehabilitation medicine team started a pilot programme at the Ang Mo Kio Rehabilitation Centre to provide specialised, intensive and advanced service to wean patients off their reliance on ventilators early and restore them to health.
Snoring disrupts sleep not just for the sufferer but also for their partner. While a nighttime symphony of sniffles and snorts might seem minor, it could signal a more serious underlying condition: sleep apnea. This article delves beyond the disruptive sounds of snoring to explore the realities of sleep apnea, its potential health risks, and the importance of seeking timely treatment.
Understanding Sleep Apnea: More Than Just Snoring
Sleep apnea is a prevalent sleep disorder characterized by repeated pauses in breathing throughout the night. These pauses can last for seconds or even minutes, causing the brain to wake up to restart breathing briefly. Individuals with sleep apnea often experience frequent nighttime awakenings, even if they’re unaware of them, leading to fragmented sleep and daytime fatigue.
There are two main types of sleep apnea:
Obstructive sleep apnea (OSA) is the most common type, caused by a blockage of the airway during sleep. Relaxed throat muscles or enlarged tissues can obstruct the airway, leading to breathing pauses.
Central sleep apnea is less common when the brain fails to signal to breathing muscles.
Symptoms and Risks of Untreated Sleep Apnea
While loud snoring is a common symptom of sleep apnea, it’s not always present. Here are some other signs and symptoms to watch out for:
Excessive daytime sleepiness (EDS): Feeling constantly tired and struggling to stay awake during the day.
Witnessed apneas: A partner observing periods where your breathing stops and restarts.
Morning headaches: Waking up with a persistent headache upon arising.
Restless sleep: Experiencing frequent tossing and turning throughout the night.
Mood changes: Increased irritability, difficulty concentrating, or feeling depressed.
Untreated sleep apnea poses significant health risks. Here’s why seeking timely diagnosis and treatment is crucial:
Increased risk of heart disease: Sleep apnea can contribute to high blood pressure, irregular heartbeats, and an increased risk of heart attack and stroke.
Metabolic issues: Sleep apnea can disrupt hormones that regulate blood sugar, potentially leading to type 2 diabetes.
Cognitive decline: Fragmented sleep due to sleep apnea can impair memory, focus, and overall cognitive function.
Increased risk of accidents: Daytime sleepiness associated with sleep apnea can significantly increase the risk of accidents while driving or operating machinery.
Taking Action: Diagnosing and Treating Sleep Apnea
If you suspect you or your partner might have sleep apnea, it’s crucial to seek medical attention. Diagnosis typically involves a sleep study, in which you spend the night in a specialized facility monitored for breathing patterns, oxygen levels, and brain activity.
Here are some standard treatment options for sleep apnea:
Continuous positive airway pressure (CPAP): This is the most common treatment, utilizing a mask worn during sleep that delivers a constant stream of air to keep the airway open.
Oral appliance therapy: Sometimes, a custom-made mouthguard can be worn at night to help maintain an open airway.
Surgery: In severe cases, surgery might be necessary to remove or reshape tissues blocking the airway.
Prioritizing Sleep Health: A Sound Investment in Your Well-being
Sleep apnea is a treatable condition, but timely diagnosis and intervention are crucial. Ignoring the problem can have severe consequences for your overall health and well-being. Here are some key takeaways:
Don’t dismiss loud snoring: While not everyone who snores has sleep apnea, persistent snoring warrants a visit to your doctor.
Be aware of the symptoms: Daytime fatigue, frequent awakenings, and morning headaches could be signs of sleep apnea.
Seek professional diagnosis: A sleep study is the most effective way to diagnose sleep apnea and determine the appropriate treatment course.
Treatment improves quality of life: Addressing sleep apnea can significantly improve your sleep quality, energy levels, and overall health.
By prioritizing sleep health and seeking professional help if you suspect sleep apnea, you can reclaim restorative sleep, reduce your risk of chronic health problems, and improve your overall quality of life. Remember, a good night’s sleep is an investment in your well-being, and addressing sleep apnea is a critical step towards achieving a healthier, happier you.
Serene beautiful woman sleeping with hand under cheek on soft pillow, young female wearing white pajamas resting under warm blanket in comfortable bed in bedroom or in hotel, enjoying sweet dreams
Fizkes / Getty Images
While most phone apps are perfectly fine as the free versions, sometimes people find a paid phone app with features that just knock things out of the park. So, I asked the BuzzFeed Community to tell us the phone app they don't regret buying, and here's what they had to say below:
2.". As someone who works on spreadsheets all day, the library of podcasts and music is a necessity."
3."! It's an app full of erotic audio stories and sounds that have been incredibly helpful in my quest to 'get my groove back' or whatever after a few really stressful years shut down my sex drive. Reading erotica has never really done it for me, and porn can be so male-gaze centered that it kinda turns me off, but the stories on Dipsea are really immersive, sexy, and fun. I started with a free trial and never looked back."
—Gemma, 39, Oakland
4.". I get panic attacks constantly. I also live with chronic pain and insomnia. I love all the nighttime things. The 'falling back to sleep' is a fucking goldmine all by itself. It gives me guided meditation through crippling painsomnia. I love the little stories when I can't get my brain to shut up. The 500-minute rain is also really great, and all that is just the night stuff. The daytime gives me options for when I'm panicking, hurting, flustered, all of it. I don't use this every day, but when I need it, I'm in a very dire place. My therapist suggested it, and I ran with it. [It has been] life-changing for me. As you can tell, I'm a little high-strung."
5.". As a small business owner, this app allows me to do so much! I can create everything from product labels and signage to social media posts that all look super professional. So, so worth the $12 a month."
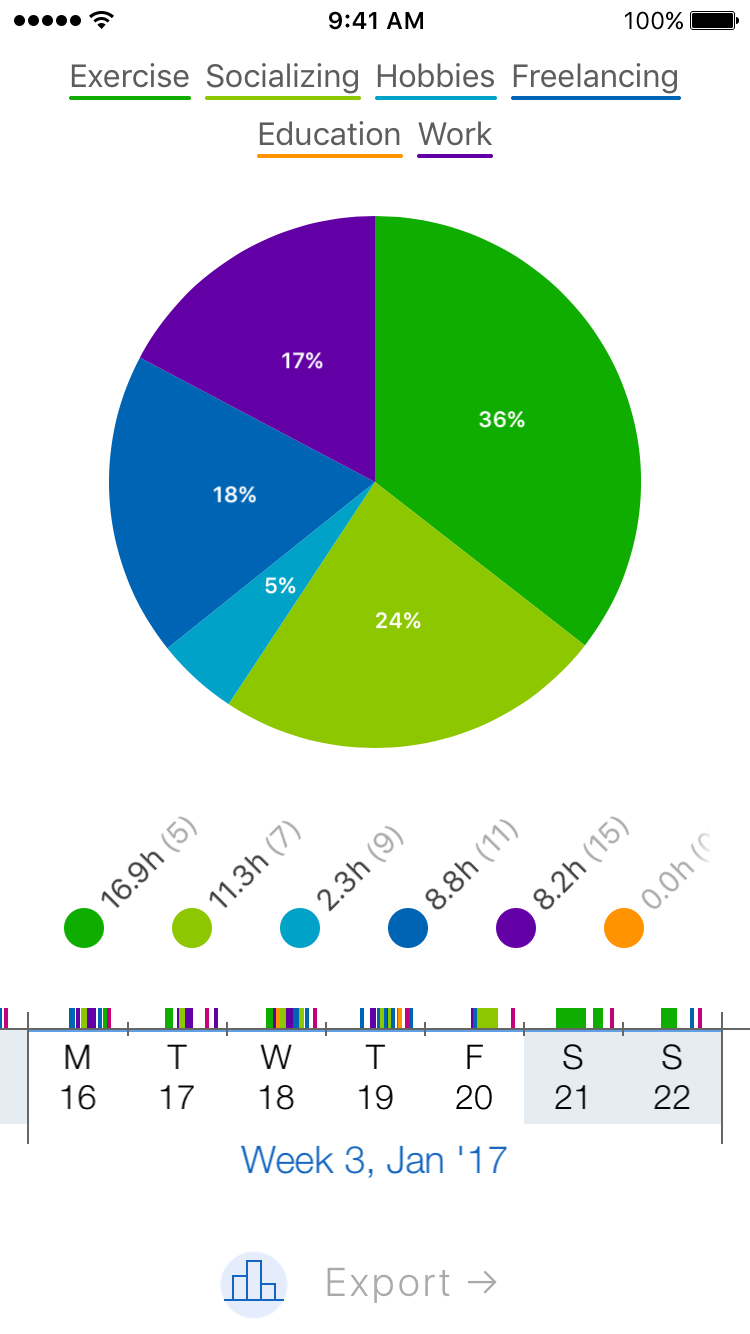
6.". I like to track the time I've spent doing different activities to help me with my time management, so I make sure I get everything done that I want and need to do. There's a free version, but with paid, you can track unlimited things. It's been so helpful!"
7.". I can't believe the time I wasted, in the beginning, keeping manual spreadsheets of money coming in, money spent, miles driven for work, etc. If you're self-employed, do yourself a favor and spend the $15 a month to use QB; it'll save so much time and frustration!"
—Anonymous, 34, Tennesse
8."If you’re actually using it regularly, is great! But I waited until I had a full year of daily practice under my belt before doing it because I’m not about to pay to have an owl shade me every day."
9."Are you kidding? . An hour after trying the free version, I knew this app would positively change my entire life! Now, five months later, I can't imagine NOT being able to verbally ask my phone a question and have it talk back with the correct answer. Too bad it wasn't around before I retired because I'd probably be the senior VP of my old company in about a year!"
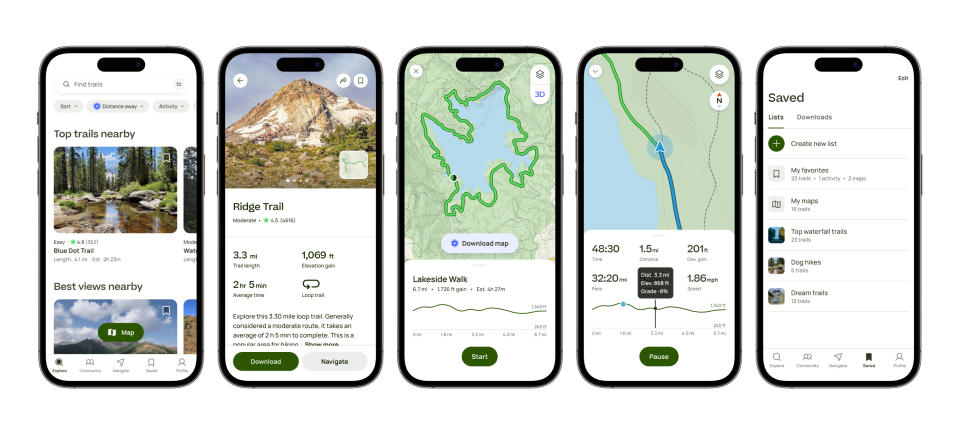
10.". It's basically a satellite navigation [app] for walking. It gives you directions to a parking spot and then navigates you on a trail. As someone who isn't a confident map reader, this app has really allowed me to go out and enjoy the outdoors without getting worried about getting lost, and it's been so good for my physical and mental health!"
11."!! My husband and I love to try new recipes. Not only are the recipes tried and true, but they are easy and always delicious! It has also become my husband's go-to destination for kitchen tools to buy. We are on our second year of the subscription and are always finding something different to try! 100% recommended for people who love to cook and want to try new things!"
—Bananer, 41, Wisconsin
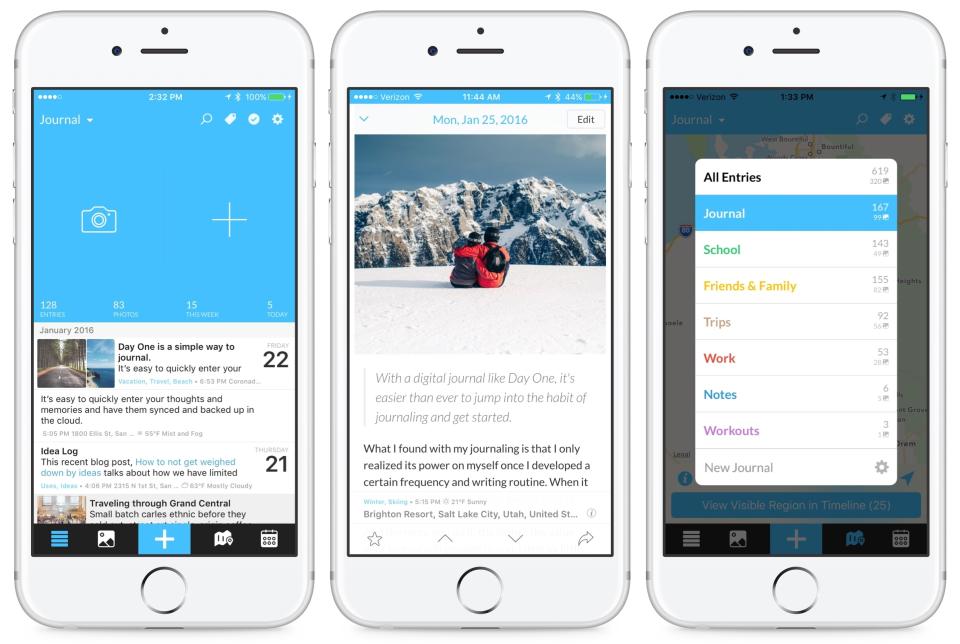
12."! I have used this journaling app for years now, and it continues to add new and exciting features all the time. It's a great way to journal via text or audio, and you can add all types of media to a journal entry. There are tons of ways to organize different topics via different journals and tags. I will never not pay for this because I use it daily!"
13."! One subscription gives you access to multiple apps for various workouts that you can customize EVERYTHING. The voice and speed of the voice telling you what to do, the music playing, the skill level, endless. It makes me want to work out; it's worth every penny."
14."! I honestly cannot sleep without the sleep stories now! I'm someone who really struggles to switch off at night, and listening to sleep stories has been so incredibly helpful. It also has mindfulness and meditation exercises that are really accessible even if you're not someone who's normally into that kind of thing. I've logged 1979 hours on it, apparently. Lol."
Do you swear by a paid phone app? Tell us what it is and why you love it in the comments below:
Holi, the festival of colours, is here, and people are all set to celebrate it with their loved ones. Though the occasion is auspicious and the moment joyful, asthmatic patients should take extra care during this time.
Asthma is a lung condition characterised by narrowing, swelling, and muscle tightening around the airways, leading to breathing difficulties, coughing, and chest pain. According to the World Health Organization (WHO), it affected 26.2 crore people in 2019 and caused 4.55 lakh deaths.
Ahead of Holi celebrations, Dr Kutty Sharada Vinod, Pulmonologist, Karuna Hospital, Delhi,shares how Holi colours can impact our respiratory health and what people with asthma can do to protect themselves.
Holi colours are not just harmless pigments; they often contain heavy metals, broken glass fragments, chemicals, and pesticides, says Dr Vinod.
According to her, heavy metals like lead can cause disabilities and are particularly dangerous for children. Chromium, another common component, can lead to bronchitis, asthma, and allergies, whereas mercury present in the colours can impact kidney, liver, and foetal health, she adds.
Dr Vinod says that the harmful components in the Holi colours can pose serious threats to your respiratory system, leading to a range of health issues.
A 2016 study published in the Journal of Occupational Medicine and Toxicology even found that Holi colour powders contained very small particles that could be inhaled deeply.
In lab experiments, these powders caused immune system cells to overreact and release inflammatory chemicals, which could explain why some people experience skin irritation, eye problems, and breathing difficulties after Holi celebrations, the researchers noted.
Protective Measures Asthma Patients Should Take
Here are some measures people with asthma can take to prevent attacks or the worsening of symptoms:
Choose natural colours: Use natural and organic colours made from ingredients like turmeric, rose powder, beetroot, and other plant-based materials. According to Dr Vinod, synthetic colours contain chemicals that can irritate the respiratory system and trigger asthma symptoms. By using natural colours, you reduce the risk of respiratory distress while still enjoying the festive spirit of Holi, she says.
Wear a mask: Before venturing out to play Holi, ensure you wear a mask or scarf that covers your mouth and nose. Use a breathable material to prevent discomfort while effectively blocking airborne particles from entering your respiratory passages.
Avoid smoke and pollution: Dr Vinod says that Holi festivities often include bonfires and the burning of Holika effigies, which can release smoke and pollutants into the air. If possible, stay indoors during these events to reduce exposure to smoke, she recommends.
Keep your inhalers handy: Asthma patients should always carry their inhalers with them, even if they feel well. The excitement and physical activity involved in playing Holi can sometimes lead to sudden asthma symptoms. It is therefore best to be prepared.
Monitor children with asthma: If your child has asthma, closely supervise their Holi activities. Ensure they use natural colours, avoid playing near smoke or bonfires, and have their inhaler readily available.
Maintain a balanced diet: During this celebratory day, do not compromise on your diet. Consume a nutritious and balanced diet that can contribute to overall respiratory health. Include foods rich in antioxidants, vitamins, and minerals to support lung function and reduce inflammation.
Take medications as directed: Continue taking your prescribed asthma medications as directed by your healthcare provider, even if you're symptom-free. Long-term control medications help prevent asthma attacks and manage underlying inflammation in the airways, says Dr Vinod.
Conclusion
Holi is a joyous festival that calls for great celebrations. However, people with asthma should be cautious during this time. Ensure that you do not strain your airways by breathing in too many colours. Make sure you choose natural, organic colours instead of synthetic colours that contain toxic chemicals. Most importantly, keep your inhalers handy so that you can use them in case you have a sudden asthma attack.
All possible measures have been taken to ensure accuracy, reliability, timeliness and authenticity of the information; however Onlymyhealth.com does not take any liability for the same. Using any information provided by the website is solely at the viewers’ discretion. In case of any medical exigencies/ persistent health issues, we advise you to seek a qualified medical practitioner before putting to use any advice/tips given by our team or any third party in form of answers/comments on the above mentioned website.
Respiratory Syncytial Virus (RSV) is a respiratory virus that commonly affects individuals of all ages but is particularly notorious for its impact on infants and young children. This article aims to provide an overview of RSV – its symptoms, transmission, prevention, and treatment, with a special focus on its effects on children.
RSV typically causes mild, cold-like symptoms in adults and older children, but can lead to severe respiratory illness in infants and younger children. The virus primarily affects the lungs and respiratory tract, leading to coughing, wheezing, difficulty in breathing, fever, and in severe cases, pneumonia or bronchiolitis.
Transmission of RSV occurs through respiratory droplets when an infected person coughs or sneezes. It also spreads through direct contact with contaminated surfaces. The virus can survive on surfaces for several hours, making it highly contagious, especially in settings like daycare centers or schools where young children gather.
RSV can be particularly concerning in infants and younger children due to their smaller airways and immature immune systems. Premature infants and those with underlying health conditions, such as congenital heart disease or chronic lung disease, are at a higher risk of developing severe complications from RSV infection.
Preventing RSV infection in children involves several strategies, including:
1. Hand hygiene: Regular handwashing with soap and water, especially before handling infants or young children, can help reduce the risk of RSV transmission.
2. Avoiding close contact with unwell individuals: Limiting exposure to people with respiratory infections, particularly during RSV season, can lower the risk of transmission.
3. Cleaning and disinfecting surfaces: Regular cleaning and disinfection of commonly touched surfaces can help prevent the spread of RSV.
4. Respiratory etiquette: Encouraging individuals to cover their mouth and nose when coughing or sneezing can help prevent the spread of respiratory droplets.
Additionally, for infants at high risk of severe RSV infection, healthcare providers may recommend prophylactic treatment with palivizumab, a monoclonal antibody that can help reduce the severity of an RSV attack.
Treatment for RSV in children focuses primarily on supportive care such as ensuring adequate hydration, maintaining airway patency, and providing supplemental oxygen if necessary. In severe cases, hospitalisation may be required for close monitoring and supportive therapy, including respiratory support.
In conclusion, the Respiratory Syncytial Virus poses a significant health risk to infants and young children, particularly those with underlying health conditions. Understanding RSV's symptoms, transmission, prevention, and treatment is crucial for parents, caregivers, and healthcare providers to mitigate its impact on child health and well-being. By implementing preventive measures and seeking prompt medical attention when necessary, the burden of RSV-related illnesses in children can be reduced.
SOLEDAD – The Correctional Training Facility (CTF) Investigative Services Unit is investigating the death of an incarcerated person who died after he attacked correctional officers during an altercation.
On March 21, 2024, at approximately 11 a.m., officers were releasing people from their cells. Incarcerated person Joseph Altamirano yelled at and then struck an officer with his fist. The officer then struck Altamirano, who fell to the ground and attempted to reengage. Staff activated their personal alarm devices, gave verbal orders to “get down” and then used pepper spray when Altamirano continued to try to assault an officer. Officers held Altamirano to the ground and put him in restraints to stop the attack.
Shortly after, Altamirano began having difficulty breathing. Staff immediately began life-saving measures and transported him via ambulance to an outside medical facility. At 12:36 p.m. Altamirano was pronounced deceased by a hospital doctor.
During the incident, Altamirano attacked one staff member. The assaulted staff member was evaluated and treated at CTF. Additionally, two responding staff members were transported to outside medical facilities. Both staff members have since been treated and released from the hospital.
Altamirano was most recently admitted from Santa Clara County on Nov. 24, 2003, to serve life with the possibility of parole for attempted carjacking and attempted kidnapping as a third-striker, with enhancements for prior felony convictions of a serious offense.
Officials have limited movement where the incident happened to facilitate the investigation. The Office of the Inspector General, the Office of Internal Affairs and CDCR’s Deadly Force Investigation Team were notified. The Coroner’s Division of the Monterey County Sheriff’s Office will determine Altamirano’s cause of death.
CTF houses minimum- and medium-security male incarcerated people. The prison opened in Monterey County in 1947, houses more than 4,000 incarcerated people and employs 1,189 staff.
We do it every day without thinking—in, out, on average 7.5 million times a year. And we think that if we just get the air into our lungs, it doesn’t matter which way it comes in. But new evidence suggests we’re doing it all wrong.
If we’re to achieve optimum health, we need to take in far more oxygen than we ordinarily do, and we need to make sure that it gets into places it’s just not reaching. The main reason we’ve got an oxygen deficiency has to do with the very way we breathe.
With all the stresses of modern life and hours spent hunched over computers or phones, our breathing has become too quick and too shallow. But as Celeste McGovern reports in The Healing Power of Breath the greatest problem has to do with the almost universally accepted idea that breathing through your mouth is equivalent to breathing through your nose.
Mouth breathing has become ubiquitous, partly due to the effect of soft processed foods on the structures of our faces, which causes our nasal airways to shrink. But taking in oxygen through our mouths, particularly at night, can be responsible for a host of illnesses, including sleep apnea, asthma, panic attacks, high blood pressure, autoimmune diseases—even mental illnesses like depression. These problems can begin in a matter of days after breathing through our mouths.
As McGovern discovered, James Nestor, author of Breath: The New Science of a Lost Art (Riverhead Books, 2020), tried out a little experiment with a colleague of his in which their noses were blocked during sleep. Within days, both began to suffer from snoring and sleep apnea.
Nestor contracted microorganisms in his nose that would have developed into a full-blown sinus infection had he carried on the experiment for more than 10 days. Both their blood pressures began to skyrocket, and their heart rate variability scores (a measure of good heart health) nosedived.
Nestor also began suffering from anxiety and high stress levels. Once he and his colleague reversed the process and taped up their mouths to sleep, all the conditions reverted back to a healthy normal in a matter of days.
Nose breathing owes its superiority to the added effect of nitric acid it produces, which delivers nearly a fifth more oxygen to the body, kills bacteria and viruses including Covid, and dilates arteries to deliver more blood and oxygen to the body, among many other effects.
In fact, learning to breathe slower and deeper through the nose can also help to heal asthma and even high blood pressure, one of the most common health problems.
The other aspect of breathing that affects our health is that we’re not getting adequate oxygen in the first place. To maintain a healthy body, we need our red blood cells to be saturated with 96–100 percent oxygen. But if our breathing is impaired in any way, as it is with emphysema and other lung diseases, like asthma, our red blood cells just don’t get enough.
Pollution and other toxins and even trauma can limit the amount of oxygen we take in, which can eventually result in all the diseases listed above and more. The good news, as Dr Leigh Erin Connealy covers in How Oxygen Therapy Can Heal Your Body and Mind, is that you can boost your levels of oxygen quickly via a hyperbaric oxygen chamber, which delivers pure oxygen to the body at two or three times the pressure in the atmosphere.
This therapy entails stepping inside a little hyperbaric chamber and breathing in oxygen while the air pressure is gently ramped up.
As Dr Connealy explains, the oxygen delivered in this way largely bypasses the red blood cells and heads directly to blood, plasma and cerebrospinal fluid, among others, flooding the body with about 15 times the usual amount of oxygen.
Although conventional treatment uses hyperbaric oxygen for certain conditions, Dr Connealy includes it in the array of treatments she uses against cancer. Because cancer cells are anaerobic (they live without oxygen), a blast of pure oxygen into the blood cells makes it harder for them to survive.
Pure oxygen delivered in this way also mitigates some of the damage wreaked by chemotherapy and radiotherapy in their indiscriminate attack on both healthy and cancerous cells. What’s more, hyperbaric oxygen cranks up the body’s production of stem cells, reduces inflammation, and gives the brain a cognitive boost by increasing cerebral blood flow.
As with breathing correctly, getting enough oxygen through a hyperbaric delivery tunes up the immune system, helping to both ward off infection and promote rapid healing. Besides hyperbaric oxygen, Dr Connealy also recommends other types of oxygen delivery, such as Cyclic Variations in Adaptive Conditioning (CVAC), which changes the oxygen pressure as it cycles through the machine, plus different types of ozone therapy (another type of therapy that infuses the blood with oxygen), oxygen baths, and oxygen and ozone combined.
The bottom line for all of this is that the most effective treatments are often the simplest. In this case, it’s a matter of making sure we have plenty of the right air and we are getting it to the right places.
Isabella Willingham, 21, a now former student at Asbury University, told NBC News Monday that neither she nor police pieced together what happened when her roommate found her unresponsive in their room with deep lacerations and bruising in November.
“I believe God spared me because my mission is to now bring light to the safety issues on campus. The students definitely need way more protection than they’re getting,” Willingham told the outlet.
Isabella “Bella” Willingham has since left the private Christian university following the strange incident in November which landed her in the hospital with deeply concerning injuries.
“I want what happened to me to draw attention to the fact that Asbury needs more cameras on all of their exits and entryways.”
Willingham told the outlet she couldn’t remember what happened to her on Nov. 27 — and the injuries were severe enough that it left her memory fragmented from most of her past semester at the university — but believes she never left her dorm room the day of the incident.
Willingham’s room was located in Glide-Crawford Residence Hall, an all-female dormitory with strict rules about men entering the building, and all visits from males were documented.
A rape kit and toxicology report from that night show that Willingham was not sexually assaulted and “found nothing of concern,” the outlet reported.
Paramedics told her parents their daughter had stopped breathing on her own for 23 minutes. LEX18
The former student said it could have been “a group” that would easily be allowed to roam the building without being questioned as she narrowed down who it could have been if she was attacked.
“It was probably a group of girls. I barely talked to anyone. I knew like three people on campus. Like, I never left my room,” she said. “I just feel like it was girls because I only knew girls.”
The 21-year-old felt “violated” over Asbury’s slow response and did not intend to return to school.
“I don’t want to go back unless the person, whoever did this, is caught,” Willingham said.
“All I can do with this is to try to expose what the school is doing and to try to protect other people on campus.”
Paramedics told her parents their daughter had stopped breathing on her own for 23 minutes. LEX18
While the incident baffled Willingham and her family, police also changed their tune about what may have happened to the young college student that night.
The Jessamine County Sherif had claimed Willingham’s injuries were most likely due to her falling out of her bunk bed or a medical episode, but those theories have been put to rest by the department.
Sheriff Kevin Grimes told the outlet Monday that a person from his office “spoke out of turn” and they are taking the investigation seriously.
“It’s 100% baffling what happened to this young lady,” Grimes said. “In some way, shape, form or fashion, she’s a victim just like anybody else. … We 100% believe something happened; we just don’t know what.”
Willingham, 21, a student at Asbury University, was rushed to the hospital on Nov. 27 and placed in intensive care due to the severity of her injuries. Facebook
His department has since spent hundreds of hours trying to piece together what happened that night, reviewing hours of camera footage and speaking with dorm residents, but the lack of evidence and the fact that no one has come forward to report anything has made it a serious challenge.
Grimes also shared that when his officers got called that night, it was reported as a potential overdose.
However, when Willingham arrived at the hospital, they were called back because of the injuries found on the lower half of her body — something his deputies did not see when they arrived on campus because she was covered.
“The one thing that we have going against us was that we did not get notified to the injuries to her legs until probably five or six hours later. … I can say we were behind the eight ball when it comes to the injury side of it,” Grimes told the outlet.
Nevertheless, Willingham expressed great gratitude for the first responders who helped her that night.
“I survived my attack, and I’m so thankful for the first responders who didn’t give up on me. I’m alive because of that,” she told the outlet.
Asbury University said that all future questions should be directed to the sheriff’s office.
Asbury University said in a statement last week that its “priority remains the safety and wellbeing of its students, faculty, and staff” and that all future questions should be directed to the sheriff’s office.
At a meeting held at Glide-Crawford dorm Sunday night, Willingham and her mother, Jennifer Willingham, and more than 100 others were told by Asbury President Kevin Brown that there was no threat to students on campus.
Hughes Memorial Auditorium at Asbury University in Kentucky. Getty Images
Brown had told the concerned attendees that the sheriff’s office “publicly confirmed that. I want to share that with you and I want to reiterate that,” according to a recording of the meeting the family provided to NBC News.
“It was like Bella was being the perpetrator. Bella was the victim who became villainized,” Jennifer Willingham said.
“If they believed my daughter was attacked, they would for sure say, ‘Guys, there’s somebody on this campus. We need to find out who did this.’”
In 2019, Rebecca Poehlmann of Dallas, Texas needed 26 medications to manage health conditions like prediabetes, fatty pancreas disease, fatty liver disease, migraines, epilepsy, irritable bowel syndrome, ovarian cysts, blood pressure, anxiety and depression. She needed additional medication to manage the side effects of all the drugs.
“I was in so much physical pain and mental pain. Everything hurt. It hurt to walk. It hurt to sleep,” she tells TODAY.com.
“My brother started getting concerned. He wanted to take walks with me, but I was so heavy I turned him down. I would go back to bed. My dad, who was a doctor, also voiced his concerns. My doctors were worried about me. They warned me I could die of a stroke or heart attack, but I wasn’t listening. I had given up.”
After losing her brother and father, Rebecca Poehlmann's weight climbed to 285 pounds. (Courtesy Rebecca Poehlmann)
In December 2019, Poehlmann’s brother and father passed away within a week of each other. “After that, I turned to food for comfort and gained another 30 pounds,” she says. Her weight climbed to 285 pounds.
Her husband finally said, ‘Honey, I think your weight is going to kill you. And I can’t live this life without you.’ My brother, my dad and my husband, the three most important people in my life, had all told me they were worried I was going to die. I had to do something,” she says.
Poehlmann, 44, decided to have weight-loss surgery, which turned her life around. She lost 150 pounds and put on muscle weight, reversed prediabetes, fatty liver disease and fatty pancreas, and no longer needs medication for high blood pressure. She’s down to just six medications.
“I can tie my shoes now. I can fit into my shower now. I can sleep without pain and suffering. I don’t fear having a stroke or heart attack at any minute and leaving my husband a widower,” she says.
And she says it’s the improvements she’s seen in her mental health and her fitness that have transformed her life: “I came from a very dark place, and now I’m living my best life.”
Here’s how she did it.
At one point, Rebecca Poehlmann was on 26 medications to manage health conditions like prediabetes, fatty liver disease, migraines, blood pressure and depression. (Courtesy Rebecca Poehlmann)
Weight-loss surgery got her started
In December 2020, Poehlmann had gastric sleeve surgery. She points out that weight-loss surgery isn’t the easy way out: “At first, it felt impossible.”
And managing her diet with a very small stomach is challenging. “At first, you go from overeating to just having liquids. You basically have no stomach,” she says.
Now she drinks two large protein shakes a day since she needs 80 grams of protein daily. She has five small meals, and in between, she aims to drink 80 ounces of water. She can’t drink water 30 minutes before or after a meal because it will fill up her stomach.
She needs to focus mainly on protein, with minimal carbs or fat. She eats shrimp, fish, tofu and sushi and tries to eat some chicken and steak.
She’s pleased with her progress, but she’s dealing with an unwelcome side effect: loose skin. She would like to have surgery to remove it, but she estimates that would cost $50,000, and her insurance does not cover it. “I’m about 90% happy with myself. If I had the plastic surgery, I would be 100% happy with myself.”
Gastric sleeve surgery helped kick off Poehlmann's weight loss, but learning how to eat healthfully and exercise were key for losing weight and keeping it off. (Courtesy Rebecca Poehlmann)
She focused on fitness with walking and strength training
Poehlmann joined Life Time on New Year’s Eve, 2020, and she was in tears, crying to the head coach: “I said, ‘I can’t do this. There’s no way I’m going to take off all this weight.’ She said, ‘You can and you will do this.’”
As Poehlmann started going to the gym, she felt like she found a second family. “We all support each other,” she says.
At first, she would walk and learn how to complete exercises correctly. She slowly built her fitness. Now she spends an hour in the gym Monday through Friday, taking a class called GTX that’s half weightlifting and half cardio. After that, she spends an hour in recovery with air compression massage or water massage.
Poehlmann says she felt like she found a second family at Life Time Fitness. (Courtesy Rebecca Poehlmann)
“Now I can do 250 squats with 80 pounds on my shoulders. I can do all sorts of planks, and I didn’t even know there were so many kinds of pushups. I can do burpees, box jumps, bosu planks and power cleans. I never believed I would ever have this much muscle. I never thought in my life that I could do these things. I feel so accomplished every time I leave that gym.”
Her fitness extends beyond the gym. She can go parasailing and ride horses again. “There are so many things that have weight restrictions. If you’re anywhere close to 300 pounds, you can’t ride a horse. I like being able to do these things again.”
She’s been surfing, and she’s training to hike the Grand Canyon and to run a half-marathon. “Fitness is a huge part of my life. I’m doing things I never thought I’d be able to do,” she says.
After losing 150 pounds, Poehlmann has picked up hobbies like surfing, horseback riding and parasailing. (Courtesy Rebecca Poehlmann)
Her mental health improved along with her physical health
“Society is mean to obese people. And there’s so much shame. Even now, I have shame that I ever got that big. People who are heavy carry a lot of shame and a lot of embarrassment. They lock themselves away, and they isolate and that leads to really bad depression. That’s exactly what I did,” Poehlmann says. “I had given up on life. I didn’t like myself. I was even suicidal when I was heavy. It was bad. Everyone was worried about me.”
At one point, Poehlmann’s best friend took her to Florida. On that trip, she told Poehlmann she was a good person with a good heart. “That resonated with me, and I started to find self-love when I was heavy,” she says.
Now, she feels transformed: “I’m a different person now. I’m hopeful for my future. I know that I’m going to keep this healthy lifestyle. My mental health is just so improved. I’ve never been happier in my entire life. I didn’t know that it was going to take me 44 years to get here, but I got here. And now I’m this person who’s on top of the world.”
Once contemplating suicide, Poehlmann’s new lifestyle has transformed her mental health.
This article was originally published on TODAY.com
It appears that the vagus nerve has hired a publicist. A brief foray on TikTok reveals that the previously introverted nerve, said to assuage anxiety when activated (a claim often made through injected lips in a hushed vocal fry) is having its day.
Likewise, the moon has hired a social-media consultant. If ever there were so many varieties of a full moon (blood, cold, pink, super, beaver, micro), never has the quantity of accompanying healing modalities (manifesting, crystal charging, intention setting, sound bathing) been greater.
Timing is everything. But what if one’s cacao ceremony conflicts with one’s intermittent fast? And then there’s the problem of breath work. To Wim Hof or not to Wim Hof? To box breathe or breathe coherently? I just need to know the perfect way to breathe. Especially in a time of crisis.
In 2023, I lost two friends to suicide and got scared that it was contagious. Overcome by the natural symptoms of grief—fatigue, heaviness, panic, existential questioning—I worried that my usual levels of depression and anxiety (considerable) had spawned a new species of depression and anxiety babies. Worse still, the babies seemed to be growing.
For nine months, I attempted to heal myself. I read self-help books: David D. Burns’s Feeling Good, Claire Weekes’s Hope and Help for Your Nerves, and Eckhart Tolle’s The Power of Now. I read spiritual books: Shunryu Suzuki’s Zen Mind,Beginner’s Mind, Thich Nhat Hanh’s Peace Is Every Step, and Alan Watts’s Still the Mind. I changed therapists. I changed psychiatrists. I changed antidepressants. I changed antidepressants again. I transitioned my 17-year meditation practice from a transcendental modality to a vipassana style. I saw a healer on Zoom. I saw a psychic in person. I entered an intensive outpatient program for depression and anxiety. The program seemed to make me worse. I tried somatic therapy. Internal Family Systems. Box breathing. 4-7-8 breathing. Progesterone. Judson Brewer’s Unwinding Anxiety app. Praying to angels. And, yes, activating the vagus nerve.
I undertook each of these actions under the auspices of learning to “sit with” negative thoughts and feelings. Truthfully, I wanted the thoughts and feelings expunged. I’d heard it said that “what you can feel you can heal” and that “the only way out is through.” But when, I wondered, would through be through? When would I finally be well? After nine months, all my “healing” led to was a hypervigilance so severe that I had to enter an outpatient program for obsessive-compulsive disorder. The obsession? My own mental health. The compulsion? Trying to fix it.
Thomas Albdorf
My most recent mental-health and wellness odyssey echoes a larger American phenomenon. As a culture, we are more preoccupied with our mental health and well-being than ever, thanks to relentless messaging and marketing of seemingly endless products, apps, and supplements that would have us believe that being “well” has an end point. It doesn’t, of course, but it’s a very lucrative proposition. Researchers at McKinsey & Company recently estimated the value of the global wellness market at $1.8 trillion and expect it to grow 5 to 10 percent each year in the U.S. alone. Moreover, we are more therapized than ever … and still more anxious and depressed than ever.
The Centers for Disease Control and Prevention reported that in 2020, 20.3 percent of American adults surveyed had received mental-health treatment in the past 12 months and 16.5 percent had taken prescription medication for their mental health. In October 2023, according to the U.S. Census Bureau’s Household Pulse Survey, 34.2 percent of adults reported anxiety and/or depression symptoms.
The cult of physical- and mental-wellness culture prescribed by Goop, Erewhon, Moon Juice, and other exclusive outfits touting costly products ($1,999 far-infrared hot-gemstone mat, anyone?) equates wellness with moral goodness; this is nothing new. Yet a simple Google search for the word depression yields sponsored links for such products in the mass market as well. A company called Joyous offers very-low-dose ketamine treatment for $129 a month and asserts, “You deserve to thrive, not merely survive.” Online therapy platform BetterHelp states, “You deserve to be happy.” A “Feel Your Feelings” T-shirt is available on Amazon for $16.99. Goop now lines the shelves at Target.
When wellness is marketed as a product to be purchased, what does healing mean? And what should our expectations be?
I believe that the increased accessibility of tools and resources for mental health and well-being is, in and of itself, a good thing. But when happiness is marketed as a finite destination to be reached (often as soon as possible) and wellness as a product to be purchased, what does healing mean? And what should our expectations be?
“In our neoliberal, consumerist, capitalist culture, ‘healing’ has come to mean a hyperfocus on the individual self, almost to the point of abstraction of everything else,” says Amy Jones, a psychotherapist in New York City. “Social health, cultural health, and environmental health get ignored while we overly focus on our own individual stories, individual journey, and individual psyche, and I think that it is obviously not working very well. The individual has been the primary construct in our culture for a very long time, and that is reinforced by a lot of trends that are adjacent to healing culture: New Age spirituality, consumerism.”
Author Nada Alic echoes these ideas in “Earth to Lydia”—a short story that’s part of her 2022 collection, Bad Thoughts, which tells the tale of one woman’s journey in a dehealing group for people who have become too enlightened, too obsessively mindful.
“GET OUT OF THE PRESENT MOMENT!!” reads a flyer advertising the dehealing group on a local community board. In Alic’s story, symptoms of being so enlightened that one is no longer a part of society include “sudden preference for breathable cotton wares, bralessness where there were once bras, newfound fascination with the breath, loss of appetite, loss of libido, loss of guilty pleasures, poor hygiene, boring personality, [and] access to spirit world/other dimensions.”
Alic says the story was inspired by her own journey through New Age spirituality with an American, individualistic lens.
“I discovered Buddhism like every teen does in the early aughts, by way of dabbling in the occult and becoming obsessed with New Age spirituality as a way to cope with my undiagnosed depression and anxiety,” she says. “I collected spiritual teachers like Alan Watts and Krishnamurti like they were Pokémon and started meditating and performatively reading texts like the Tao Te Ching. I liked the feeling of participating in something ancient and universal while also getting hyperspecific personality-quiz-style answers about myself.”
If wellness is positioned as a goal—something to win at—it may actually be unhealthy. “Without problems, without discomfort, you cannot feel comfort,” says Hairan Yu, a licensed acupuncturist at Aya Acupuncture & Herbs in Los Angeles. “This is the idea of yin and yang. If you are always in a state of joy, you won’t feel it. Right now in Western society, everyone is juiced up. You need to make more money. You need to be healthier. You have to do something. If you don’t do something, you’ll feel panic. If you don’t do something, you’ll die. So people get used to thinking the rush is healthy. But that’s not healthy. Healthy is when you don’t feel a problem.”
Yu goes on to explain that healing is not something that happens in a vacuum when you’re alone, hunched over a phone on an app or in a book—at least not if the teachings in that book aren’t integrated into your life. “Healing is just a step in life,” he says. “It’s not the ultimate destination. The goal of being healthy is so that we can do everything we love to do. When we put ourselves in that state, we forget about our body. We are stepping away and letting our body fulfill our passion.”
But what about when one’s passion becomes self-healing? The Chakra Activation Meditation at Liberate Yourself, a Los Angeles wellness venue and emporium with outposts in Los Feliz and Sherman Oaks, promises to align me with my “soul’s purpose” in just 45 minutes. Such urgency! Who am I to deny my chakras (let alone my soul) when all can be fixed in under an hour?
Eda Gorbis, a psychologist and psychotherapist and the founder and executive director of the Westwood Institute for Anxiety Disorders in Los Angeles, where I went for OCD treatment, is skeptical.
“No, you cannot heal,” she says of OCD centered on mental health and wellness. “Just go and live, and then you’ll heal. To heal is to go and do it, and then you’ll change it.”
Gorbis, an immigrant from Georgia, was inspired to become a psychologist when her father—a businessman—was placed under house arrest for political reasons and their home was surrounded daily by KGB agents.
“He would say, ‘My government protects me,’ instead of being petrified. He was not afraid. And I wanted to know why some people were afraid of everything and he was not.”
But despite her profession, Gorbis laments what she sees as an American “addiction” to mental-health professionals. “A little bit of stress and they go to the psychiatrist,” she says. “Stop going to the psychiatrist every day. In Georgia, we went to our friends and neighbors, not to a therapist. I find it so interesting that people do not know their neighbors here. It is amazing that they don’t. Our neighbors in Georgia were our closest friends, and we would spend our teatime together. The door never closed. People always came and stayed, and if they had any troubles, any sorrows, any upcoming great event, they would share, and they would always seek advice from their neighbors.”
There is also, in therapeutic circles, an old notion that our therapists, spiritual teachers, and gurus should not be anything like our neighbors. In other words, that they should be a blank slate—inhuman or superhuman beings who exist on a higher plane. This leaves little room for interpersonal connection and creates more of a leader-disciple dynamic. It also precludes the possibility that the wounded healer has something to offer.
“This idea that a psychotherapist should be a totally subjective observer or mirror for a patient’s experience is very rooted in the field of psychoanalysis’s early obsession with being considered a hard medical science,” says Jones. “I don’t think that we, as healers, should be regularly taking the people who seek us out for help into any territory that we haven’t delved into and thoroughly explored for ourselves. And, because healing practitioners are of course human beings, we are all vulnerable to encountering blind spots in ourselves.”
When we’re in the pits of depression, we may be blinded by our desire to believe in something (like a “Channeling Light: Connect to the Spiritual World in 3 Parts” workshop or the notion that EFT tapping will release 44 years of emotional stress in a 50-minute hour).
Yu suggests avoiding approaching healers from a place of desperation. “There is a Chinese expression,” he says: “A drowning man will clutch at a straw.”
Likewise, a drowning man will clutch at a self-optimization podcast. Or a mindfulness app. Or a container of adaptogenic Brain Dust for $38.
As someone with OCD focused on mental health, I find the notion of trusting myself terrifying (if it’s even possible). OCD has been described as the “malady of doubt,” and what its sufferers often want most is reassurance.
What I was seeking, in my recent mental-health odyssey (which I’d never intended to be an odyssey but rather a single-stop destination), was certitude: a guarantee that I was safe from the fate that had befallen my friends. Yet as I held a rubber knife to my neck as an exposure-therapy exercise, it dawned on me that no amount of mental-health ebooks or breathing techniques or mindfulness apps had clarified whether the thoughts of suicide that looped in my mind were depressive ideation or an obsessive fear of the act. Months later, I still don’t know.
It can be helpful to remember that you are simply there existing and that that is enough. “ ‘Being’ well doesn’t necessarily mean ‘feeling’ well all the time, like the difference between happiness and contentment. We want to go for something sustainable, not chase a shiny cure,” says Susanna Brisk, a coach, healer, and certified sex educator in Los Angeles. “As a graduate of much therapy, I can attest to a frustration with the concept of ‘self-love.’ For so many years I was like, ‘Hmm, that sounds awesome, but how?’ It seemed like science fiction to get to self-love from the places I’d been. I spent years just working to attain a ‘neutral’ relationship with myself, just like, ‘I’m here. I’m safe.’ If some days you can only attain beingness rather than ‘wellness,’ that’s perfectly fine.”
If you or someone you know is considering suicide, contact the 988 Suicide & Crisis Lifeline by calling or texting 988, or go to 988lifeline.org.
It appears that the vagus nerve has hired a publicist. A brief foray on TikTok reveals that the previously introverted nerve, said to assuage anxiety when activated (a claim often made through injected lips in a hushed vocal fry) is having its day.
Likewise, the moon has hired a social-media consultant. If ever there were so many varieties of a full moon (blood, cold, pink, super, beaver, micro), never has the quantity of accompanying healing modalities (manifesting, crystal charging, intention setting, sound bathing) been greater.
Timing is everything. But what if one’s cacao ceremony conflicts with one’s intermittent fast? And then there’s the problem of breath work. To Wim Hof or not to Wim Hof? To box breathe or breathe coherently? I just need to know the perfect way to breathe. Especially in a time of crisis.
In 2023, I lost two friends to suicide and got scared that it was contagious. Overcome by the natural symptoms of grief—fatigue, heaviness, panic, existential questioning—I worried that my usual levels of depression and anxiety (considerable) had spawned a new species of depression and anxiety babies. Worse still, the babies seemed to be growing.
For nine months, I attempted to heal myself. I read self-help books: David D. Burns’s Feeling Good, Claire Weekes’s Hope and Help for Your Nerves, and Eckhart Tolle’s The Power of Now. I read spiritual books: Shunryu Suzuki’s Zen Mind,Beginner’s Mind, Thich Nhat Hanh’s Peace Is Every Step, and Alan Watts’s Still the Mind. I changed therapists. I changed psychiatrists. I changed antidepressants. I changed antidepressants again. I transitioned my 17-year meditation practice from a transcendental modality to a vipassana style. I saw a healer on Zoom. I saw a psychic in person. I entered an intensive outpatient program for depression and anxiety. The program seemed to make me worse. I tried somatic therapy. Internal Family Systems. Box breathing. 4-7-8 breathing. Progesterone. Judson Brewer’s Unwinding Anxiety app. Praying to angels. And, yes, activating the vagus nerve.
I undertook each of these actions under the auspices of learning to “sit with” negative thoughts and feelings. Truthfully, I wanted the thoughts and feelings expunged. I’d heard it said that “what you can feel you can heal” and that “the only way out is through.” But when, I wondered, would through be through? When would I finally be well? After nine months, all my “healing” led to was a hypervigilance so severe that I had to enter an outpatient program for obsessive-compulsive disorder. The obsession? My own mental health. The compulsion? Trying to fix it.
Thomas Albdorf
My most recent mental-health and wellness odyssey echoes a larger American phenomenon. As a culture, we are more preoccupied with our mental health and well-being than ever, thanks to relentless messaging and marketing of seemingly endless products, apps, and supplements that would have us believe that being “well” has an end point. It doesn’t, of course, but it’s a very lucrative proposition. Researchers at McKinsey & Company recently estimated the value of the global wellness market at $1.8 trillion and expect it to grow 5 to 10 percent each year in the U.S. alone. Moreover, we are more therapized than ever … and still more anxious and depressed than ever.
The Centers for Disease Control and Prevention reported that in 2020, 20.3 percent of American adults surveyed had received mental-health treatment in the past 12 months and 16.5 percent had taken prescription medication for their mental health. In October 2023, according to the U.S. Census Bureau’s Household Pulse Survey, 34.2 percent of adults reported anxiety and/or depression symptoms.
The cult of physical- and mental-wellness culture prescribed by Goop, Erewhon, Moon Juice, and other exclusive outfits touting costly products ($1,999 far-infrared hot-gemstone mat, anyone?) equates wellness with moral goodness; this is nothing new. Yet a simple Google search for the word depression yields sponsored links for such products in the mass market as well. A company called Joyous offers very-low-dose ketamine treatment for $129 a month and asserts, “You deserve to thrive, not merely survive.” Online therapy platform BetterHelp states, “You deserve to be happy.” A “Feel Your Feelings” T-shirt is available on Amazon for $16.99. Goop now lines the shelves at Target.
I believe that the increased accessibility of tools and resources for mental health and well-being is, in and of itself, a good thing. But when happiness is marketed as a finite destination to be reached (often as soon as possible) and wellness as a product to be purchased, what does healing mean? And what should our expectations be?
“In our neoliberal, consumerist, capitalist culture, ‘healing’ has come to mean a hyperfocus on the individual self, almost to the point of abstraction of everything else,” says Amy Jones, a psychotherapist in New York City. “Social health, cultural health, and environmental health get ignored while we overly focus on our own individual stories, individual journey, and individual psyche, and I think that it is obviously not working very well. The individual has been the primary construct in our culture for a very long time, and that is reinforced by a lot of trends that are adjacent to healing culture: New Age spirituality, consumerism.”
Author Nada Alic echoes these ideas in “Earth to Lydia”—a short story that’s part of her 2022 collection, Bad Thoughts, which tells the tale of one woman’s journey in a dehealing group for people who have become too enlightened, too obsessively mindful.
“GET OUT OF THE PRESENT MOMENT!!” reads a flyer advertising the dehealing group on a local community board. In Alic’s story, symptoms of being so enlightened that one is no longer a part of society include “sudden preference for breathable cotton wares, bralessness where there were once bras, newfound fascination with the breath, loss of appetite, loss of libido, loss of guilty pleasures, poor hygiene, boring personality, [and] access to spirit world/other dimensions.”
Alic says the story was inspired by her own journey through New Age spirituality with an American, individualistic lens.
“I discovered Buddhism like every teen does in the early aughts, by way of dabbling in the occult and becoming obsessed with New Age spirituality as a way to cope with my undiagnosed depression and anxiety,” she says. “I collected spiritual teachers like Alan Watts and Krishnamurti like they were Pokémon and started meditating and performatively reading texts like the Tao Te Ching. I liked the feeling of participating in something ancient and universal while also getting hyperspecific personality-quiz-style answers about myself.”
Thomas Albdorf - Hearst Owned
If wellness is positioned as a goal—something to win at—it may actually be unhealthy. “Without problems, without discomfort, you cannot feel comfort,” says Hairan Yu, a licensed acupuncturist at Aya Acupuncture & Herbs in Los Angeles. “This is the idea of yin and yang. If you are always in a state of joy, you won’t feel it. Right now in Western society, everyone is juiced up. You need to make more money. You need to be healthier. You have to do something. If you don’t do something, you’ll feel panic. If you don’t do something, you’ll die. So people get used to thinking the rush is healthy. But that’s not healthy. Healthy is when you don’t feel a problem.”
Yu goes on to explain that healing is not something that happens in a vacuum when you’re alone, hunched over a phone on an app or in a book—at least not if the teachings in that book aren’t integrated into your life. “Healing is just a step in life,” he says. “It’s not the ultimate destination. The goal of being healthy is so that we can do everything we love to do. When we put ourselves in that state, we forget about our body. We are stepping away and letting our body fulfill our passion.”
But what about when one’s passion becomes self-healing? The Chakra Activation Meditation at Liberate Yourself, a Los Angeles wellness venue and emporium with outposts in Los Feliz and Sherman Oaks, promises to align me with my “soul’s purpose” in just 45 minutes. Such urgency! Who am I to deny my chakras (let alone my soul) when all can be fixed in under an hour?
Eda Gorbis, a psychologist and psychotherapist and the founder and executive director of the Westwood Institute for Anxiety Disorders in Los Angeles, where I went for OCD treatment, is skeptical.
“No, you cannot heal,” she says of OCD centered on mental health and wellness. “Just go and live, and then you’ll heal. To heal is to go and do it, and then you’ll change it.”
Gorbis, an immigrant from Georgia, was inspired to become a psychologist when her father—a businessman—was placed under house arrest for political reasons and their home was surrounded daily by KGB agents.
“He would say, ‘My government protects me,’ instead of being petrified. He was not afraid. And I wanted to know why some people were afraid of everything and he was not.”
But despite her profession, Gorbis laments what she sees as an American “addiction” to mental-health professionals. “A little bit of stress and they go to the psychiatrist,” she says. “Stop going to the psychiatrist every day. In Georgia, we went to our friends and neighbors, not to a therapist. I find it so interesting that people do not know their neighbors here. It is amazing that they don’t. Our neighbors in Georgia were our closest friends, and we would spend our teatime together. The door never closed. People always came and stayed, and if they had any troubles, any sorrows, any upcoming great event, they would share, and they would always seek advice from their neighbors.”
There is also, in therapeutic circles, an old notion that our therapists, spiritual teachers, and gurus should not be anything like our neighbors. In other words, that they should be a blank slate—inhuman or superhuman beings who exist on a higher plane. This leaves little room for interpersonal connection and creates more of a leader-disciple dynamic. It also precludes the possibility that the wounded healer has something to offer.
“This idea that a psychotherapist should be a totally subjective observer or mirror for a patient’s experience is very rooted in the field of psychoanalysis’s early obsession with being considered a hard medical science,” says Jones. “I don’t think that we, as healers, should be regularly taking the people who seek us out for help into any territory that we haven’t delved into and thoroughly explored for ourselves. And, because healing practitioners are of course human beings, we are all vulnerable to encountering blind spots in ourselves.”
When we’re in the pits of depression, we may be blinded by our desire to believe in something (like a “Channeling Light: Connect to the Spiritual World in 3 Parts” workshop or the notion that EFT tapping will release 44 years of emotional stress in a 50-minute hour).
Yu suggests avoiding approaching healers from a place of desperation. “There is a Chinese expression,” he says: “A drowning man will clutch at a straw.”
Likewise, a drowning man will clutch at a self-optimization podcast. Or a mindfulness app. Or a container of adaptogenic Brain Dust for $38.
As someone with OCD focused on mental health, I find the notion of trusting myself terrifying (if it’s even possible). OCD has been described as the “malady of doubt,” and what its sufferers often want most is reassurance.
What I was seeking, in my recent mental-health odyssey (which I’d never intended to be an odyssey but rather a single-stop destination), was certitude: a guarantee that I was safe from the fate that had befallen my friends. Yet as I held a rubber knife to my neck as an exposure-therapy exercise, it dawned on me that no amount of mental-health ebooks or breathing techniques or mindfulness apps had clarified whether the thoughts of suicide that looped in my mind were depressive ideation or an obsessive fear of the act. Months later, I still don’t know.
It can be helpful to remember that you are simply there existing and that that is enough. “ ‘Being’ well doesn’t necessarily mean ‘feeling’ well all the time, like the difference between happiness and contentment. We want to go for something sustainable, not chase a shiny cure,” says Susanna Brisk, a coach, healer, and certified sex educator in Los Angeles. “As a graduate of much therapy, I can attest to a frustration with the concept of ‘self-love.’ For so many years I was like, ‘Hmm, that sounds awesome, but how?’ It seemed like science fiction to get to self-love from the places I’d been. I spent years just working to attain a ‘neutral’ relationship with myself, just like, ‘I’m here. I’m safe.’ If some days you can only attain beingness rather than ‘wellness,’ that’s perfectly fine.”
If you or someone you know is considering suicide, contact the 988 Suicide & Crisis Lifeline by calling or texting 988, or go to 988lifeline.org.
Asthma attack deaths in England and Wales are the highest they have been in the last decade and have risen by more than 33% over the last 10 years, latest figures show.
According to charity Asthma UK, more than 1,400 people died from asthma last year, an 8% increase compared to 2017.
Over 12,700 people have died from the condition in England and Wales in the last decade.
The figures also show an increase in men dying from the condition, with 436 men dying in 2018 compared to 370 the previous year.
Asthma UK is calling on the government to do more after a review commissioned by the NHS and Department for Health five years ago found that two-thirds of deaths could be prevented by better basic care.
Dr Samantha Walker, from Asthma UK, said: "I think doctors and nurses on the frontline need to make sure they're delivering these elements of basic care that are important. But equally important is that people with asthma need to make sure they're taking their preventative medicine regularly, that they have an action plan, that they know how to use their inhalers and that they know what to do in an emergency."
Eight-year-old Bailey Davis, who had mild asthma, was not called back for yearly reviews. His mother, Nicki, didn't know reviews were required, and in 2017, without warning, he suffered an acute attack and died, leaving behind his twin brother, Mason.
Nicki said: "Bailey walked into the bedroom and just said 'Mummy I can't breathe properly', but I couldn't see any visible gasping for breath so I said 'Ok darling, come on I'll give you your inhaler, give you some puffs', and he stood up and I said 'Are you ok?' In the flick of a light switch he'd gone.
"I then started CPR. My friend was downstairs and I called her to call an ambulance. I said 'Bailey isn't breathing' and my neighbours heard and came rushing in, bearing in mind Mason is still in bed, confused and shouting 'What's happening mummy? What's happening?"
Professor Jonathan Grigg, at Queen Mary University of London, puts the increase in asthma deaths down to two issues.
"The reason for this is very complicated. It's certainly on one hand to do with the environment - we're breathing in air pollution which we know makes asthma worse and actually we have new cases of asthma due to air pollution, but also our health care system is really not taking asthma as seriously as it should do."
In a statement Mike Morgan from NHS England said: "Asthma UK worked closely with the NHS to develop proposals in our Long Term Plan, which sets out measures including better diagnosis of the condition, improved medicine reviews and stronger guidance for local health services to better support families living with asthma, all of which will contribute to more than three million people benefiting from improved respiratory, stroke and cardiac services over the next decade, but as we've seen this week, with confirmation that one third of childhood asthma cases are linked to air pollution, it's clear that a big part of this challenge cannot be met by the NHS alone."
Asthma is thought to affect around 4.8 million people in England and Wales.
Breathing+ by Breathing Labs has passed peer review in a randomized controlled clinical trial that was recently published in SCI Q2 journal Pediatric Pulmonology. Research done by @bezmialem Full text is available in a link here: https://www.breathinglabs.com/clinical-trials/research-breathing-labs-and-nintendo-clinical-trial-is-published-in-journal-pediatric-pulmonology-sci-q2-impact-factor-3/?fbclid=IwAR2wNhSgurdbrrf3gzOOkHthgiWfXJ1x8RWvnMhkSo6fi33QPZEGzxzd6jM
BREAKING: @breathinglabs and @Nintendo clinical trial is published in journal Pediatric Pulmonology (SCI Q2, Impact Factor > 3), full text: https://breathinglabs.com/Nintendo%20&%20Breathing%20Labs%202022 #telemedicine #telehealth #mhealth
Clinical mouthpieces 10pcs packages are now available at 45€/50USD (shipping cost not included). Learn more: https://www.breathinglabs.com/latest-news/announcement-breathing-mouthpieces-for-clinical-and-professional-use-are-now-available/
BREATHING VR: Lately we are sourcing this VR headset for use in Breathing VR application. It allows easiest installation of both breathing+ headset cable, and USB charging cables, which is essential in professional use: https://www.banggood.com/VR-SHINECON-G5-VR-Glasses-3D-Virtual-Reality-Glasses-VR-Headset-For-iPhone-XS-11Pro-Mi10-p-1679808.html?rmmds=myorder&cur_warehouse=CN
Update: Each purchase of Breathing+ will now include three machine washable mouthpieces. Previous buyers will be supplied with those by their country representatives but will have to cover shipping costs. Please be patient while we arrange distribution. https://www.breathinglabs.com/latest-news/announcement-breathing-mouthpieces-for-clinical-and-professional-use-are-now-available/
Update: We moved servers + relocated all our games to our servers, please be patient while google reviews all that (showing unsafe website atm). Use duckduckgo or non-chromium browsers to reach our pages in the meantime. Everything ok + new product addons coming out in a month!
Registration and all functionalities at http://breathinglabs.com (and in our iOS and Android games) are fixed and fully working. If you find any issues -> [email protected]
We are back in stock with Breathing+, currently searching for VR supplier, and setting up mass production for toys and tens stimulation + in November we will be signing up new erasmus traineeships, research projects, bilateral, FP(eu), and asia-pacific ->[email protected]
BREAKING: Nintendo Co. Ltd (Japan) is implementing Breathing Games by @breathinglabs in FDA approved clinical trial for children with bronchiectasis: https://clinicaltrials.gov/ct2/show/NCT04038892
Notice to b2b partners: we are running late with some minor upgrade-> briefly running out of stock -> retail and b2b sale is closed until early october. To get a list of partners with stock to sell contact us at [email protected] Thanks, we'll go strong again in winter 💪