Introduction
Breathing, a fundamental physiological process that plays a crucial role in overall health and well-being, is often taken for granted.1 According to Nelson et al,2 the core of many breathing exercises is diaphragmatic breathing, which is considered the most fundamental demonstration of core function. These exercises involve retraining the muscles of respiration, improving ventilation, and optimizing gaseous exchange.3
Diaphragmatic breathing is recognized as a key component of many exercise protocols and practices, such as meditation, ancient eastern religions, martial arts, and yoga exercises. Diaphragmatic breathing involves the active engagement of the diaphragm to facilitate deep and efficient inhalation and exhalation. For instance, yogic breathing exercises, which originate from the yoga tradition, play a significant role in promoting relaxation, optimizing lung function, fostering emotional balance, and facilitating self-regulation.4 Many of these exercise practices and protocols not only offer diaphragmatic breathing but also incorporate other techniques such as nasal breathing, slow exhalation with pauses, smoothness, steadiness, and self-observation.
Elements of exercise programs in rehabilitation, including the ones mentioned above, have long been recognized for their significant contributions and effectiveness. This type of breathing exercises often encompasses a variety of techniques aimed at improving lung function enhancing oxygenation and strengthening the muscles involved in respiration.5–7 They play a role in helping patients recover from conditions like chronic obstructive pulmonary disease (COPD),8 asthma9 and post-surgical recuperation.10
Breathing exercises aim to improve pulmonary status, increase endurance, and enhance overall function in daily living activities.3 In particular, traditional breathing exercises such as slow breathing, pursed lip breathing, and incentive spirometry have been proven effective in enhancing respiratory capacity and alleviating symptoms associated with these conditions.11–13 However, the success of these exercises can be influenced by factors such as adherence, motivation levels and the perception of routines.14,15
Pulmonary rehabilitation (PR) in specific often involves a range of breathing exercises designed to meet the needs of patients. One example is diaphragmatic breathing exercise, which focuses on improving the efficiency of the diaphragm muscle for inhalation.16 This technique encourages deep, slow breaths to maximize lung expansion and enhance ventilation.17 Pursed lip breathing exercise also helps prevent airway collapse by maintaining positive pressure during exhalation reducing breathlessness in conditions like COPD.18 In addition, incentive spirometry devices guide patients through inhalations to increase lung capacity and clear airways after surgery.19 These exercises are crucial in pulmonary rehabilitation programs as they not only improve lung function but also help individuals regain control over their breathing.
The benefits of incorporating these exercises into rehabilitation are widely recognized. However, some people may face challenges in maintaining timing, frequency or focus on their breath during these exercises.20 Therefore, it is important to provide guidance that helps individuals maintain a breathing rhythm and awareness.
Virtual Reality (VR) technology has made advancements in recent years bringing innovative solutions to various fields, including healthcare.21 With its interactive and immersive features, VR has the potential to revolutionize breathing exercises by making them engaging and enjoyable.22 Patients can be taken to tranquil settings for guided meditation, exciting adventures, or serene landscapes by combining therapeutic breathing exercises with engaging virtual environments and scenarios.23 This combination does not help distract patients from the nature of conventional exercises but also motivates them to actively participate potentially improving their adherence to rehabilitation routines. Furthermore, real time feedback and gamified elements provided by VR enable patients to track their progress and challenge themselves making the process of enhancing function not more effective but also more enjoyable.24
VR offers an experience where patients actively participate in their rehabilitation creating a sense of presence and control. What sets VR apart is its ability to completely immerse users in environments making them feel like they are physically present in that world. This immersive nature of VR can be incredibly helpful in reducing stress and anxiety during breathing exercises.25 Many patients with conditions often feel anxious and uncomfortable due to the limitations imposed by their condition. Through the utilization of VR, patients can be sensory transported to serene and calming environments such as beaches, tranquil forests, or soothing meditation gardens. This immersive experience helps patients mentally escape from their discomforts and anxieties creating an atmosphere for effective breathing exercises and rehabilitation.25
Moreover, the interactivity offered by VR brings a level of engagement.26 This means that patients can actively take part in their rehabilitation routines while immersed in a world often mimicking real life activities. For example, they can follow the instructions of an instructor as they engage in deep breathing exercises while observing how their avatar responds within the virtual environment. The ability to interact with objects and manipulate them within these spaces fosters a sense of control which can be particularly empowering for individuals undergoing rehabilitation.27
In years, there has been a growing trend in utilizing VR to aid breathing exercise. However, there is lack of literature on how these exercises are currently incorporated into VR experiences making it challenging to evaluate their effectiveness. Particularly noteworthy is a scoping review that examines the current state of knowledge on this phenomenon. The only similar study that seems to have exist is Pancini et al study28 on the significance of VR breathing exercise in promoting mental health, while those on pulmonary rehabilitation is very limited. Additionally, it remains uncertain which rehabilitation outcomes have been accessed and whether these interventions yield results.
Literature Review
Virtual reality has grown increasingly common in healthcare intervention, notably in exercise and rehabilitation programs. The use of VR as a feasible tool for breathing exercises in rehabilitation has been examined. Numerous research has investigated the viability and efficiency of adopting VR in diverse contexts. In one study, patients with COPD employed immersive VR headsets as part of a high-intensity interval training (HIIT) exercise program.29 Twelve COPD patients took part in a six-week VR headset-based HIIT training as part of the study. Short bursts of high-intensity activity were alternated with rest or low-intensity exercise as part of the HIIT program. The patients were provided an immersive experience utilizing the VR headset, which lessened their feeling of effort and helped to inspire them. The feasibility and acceptability of VR-HIIT for COPD patients was determined by the authors. Without experiencing any serious side effects, the patients were able to conclude the HIIT program in a safe manner. Additionally, they noted that the VR experience was pleasurable and that it kept them motivated. The study’s findings show that VR-HIIT may be a novel and promising PR technique for COPD patients. Better patient results may arise from VR-HIIT’s capacity to increase desire and adherence to workout routines.
Another study examined the acceptability and safety of a VR-based deep breathing exercise for kids and teenagers getting over a concussion.30 Concussion, categorized as a mild traumatic brain injury, triggers a series of pathophysiological changes and disruptions in brain function. These effects extend to various aspects of respiratory function, such as alterations in breathing rate, mechanics, and the levels of end tidal carbon dioxide.31 Thus, fifteen participants were recruited in the study from a specialty concussion clinic within a tertiary care medical center, aged 11 to 22, who had received a concussion in the previous three months. The participants used a VR headset to pace a 5-minute deep breathing exercise. They were introduced to a serene virtual world and educated in deep breathing strategies by the VR experience. Participants discussed their experiences and any changes in their symptoms following the activity. The outcomes demonstrated that the participants considered the VR-based deep breathing exercise to be both safe and well-tolerated. None of the participants quit the workout or complained of acute discomfort. Three individuals noticed a small increase in headache, nausea, or dizziness; however, these symptoms were simply transient and did not call for medical treatment.
VR gaming and exergaming-based therapies were found to have weak to insignificant effects on heart rate and oxygen saturation in individuals with respiratory difficulties, and to have minor impacts on dyspnea, according to a systematic review and meta-analysis.32 Seventy-nine people with a range of respiratory conditions, such as cystic fibrosis, asthma, and chronic obstructive pulmonary disease (COPD), participated in the evaluation’s 19 trials. The meta-analysis’s findings demonstrated that VR exercise helped people with respiratory disorders improve their quality of life, capacity for activity, and dyspnea. Although the effect sizes were statistically significant, they ranged from low to moderate. The authors concluded that VR exercise is a practical new approach to exercise therapy for those with respiratory issues.
Furthermore, it was discovered that practicing breathing exercises with a VR system that offers multimodal biofeedback-including tactile and visual feedback-was both entertaining and successful.33 Twelve people took part in the study and used the VR equipment to conduct eight sessions of slow breathing exercises. The VR device guided the participants’ respiration with both physical and visual input. When they breathed appropriately, the participants could feel a slight vibration on their abdomen and view a virtual depiction of their own abdomen. The study’s findings demonstrated how well the multimodal VR system guided the participants’ deep, steady breathing. Following the completion of the slow breathing exercises, the participants’ breathing rate dramatically dropped. The VR system, according to the participants, improved the workouts’ motivation and enjoyment. The multimodal VR system is a viable and promising method of delivering slow breathing exercises, according to the research’s conclusion.
The findings of these studies, collectively, demonstrate the immense potential of VR breathing exercises as a cutting-edge method for managing respiratory health and rehabilitation. Further research is required to examine the wider applicability and enduring impacts of VR breathing exercises, as well as to determine the most efficient VR therapies for specific medical conditions and demographics.
Research Question
This paper provides a scoping review of existing knowledge on the possibilities of integrating VR exercise in breathing rehabilitation. Therefore, this paper aim to provide answer to this research question: “Does VR Based Exercise Therapy Offer Significant Improvement in Patients/Participant Breathing rehabilitation/Function?”
Materials and Methods
Methodology
Scoping reviews are undertaken with the purpose of delineating and examining emerging concepts within a particular field of research.34 In contrast to conventional systematic reviews that focus on narrower research issues and have a well-defined pool of relevant studies, scoping reviews are employed to explore emerging research domains and elucidate fundamental concepts.35
Search Strategy and Study Selection
Three electronic databases, including Web of Science, PubMed, and the Cochrane Library, were searched from October 28 to November 10, 2023. The query of the databases involves the use of the keywords “breathing rehabilitation, respiratory rehabilitation, virtual reality exercise, mixed reality exercise, and augmented reality exercise” to search their core collections. Following the search, citations were retrieved by the citation manager for reference management, while duplicate records were automatically excluded.
Inclusion and Exclusion Criteria
For this scoping review, articles were included without considering the specific research design. However, it is important to note that only studies involving human participants were considered, and studies involving animals were excluded from the review. articles published in English were included, and no English articles were excluded to avoid potential limitations associated with non-English papers. Specifically, the focus was on studies related to virtual reality exercise for breathing or respiratory rehabilitation, while studies outside the scope of this review were excluded. There were no restrictions regarding the year of publication or geographic region. However, articles that did not directly address the review question were excluded. Additionally, it is important to note that rehabilitation other than breathing was not within the scope of this review. Conference papers, systematic reviews, notes, secondary studies, and other reviews were excluded, prioritizing primary and original studies. The focus was on studies aimed at breathing functions and exercise, without specific limitations on the patient’s or participant’s condition. The emphasis was on including studies that directly contributed to the enhancement of breathing functions.
Article Selection
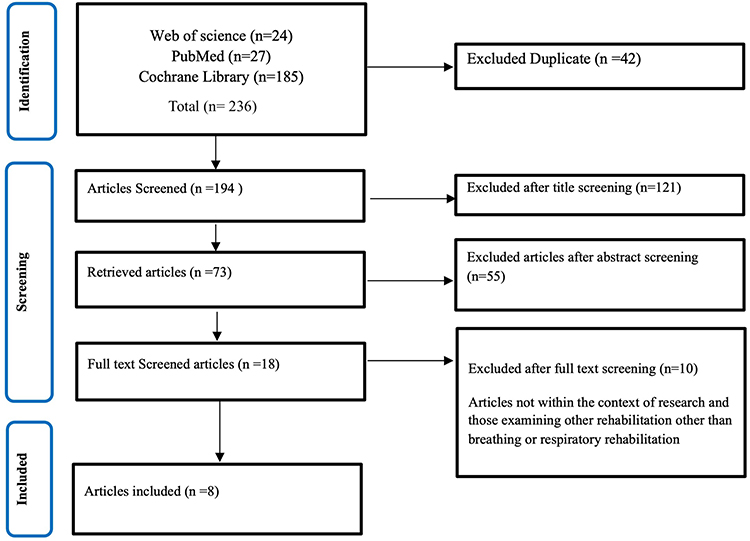
Following the retrieval of 236 citations from the databases, 42 duplicate records were removed automatically. The remaining data was then exported to Excel software version 12.0. The title and abstract of the articles were screened, and a total of 173 references were removed. The remaining 18 articles were subjected to full text screening to examine studies in line with the inclusion criteria and studies directly providing answers to the research. In this process, 10 articles not within the context of this research were excluded (Figure 1).
 |
Figure 1 Article screening flowchart.
|
Quality Assessment
The eight included studies were appraised to examine the methodological and reporting quality of these articles to rate the article’s risk of bias in planning, execution, and result presentation. In doing these, the Jonas Briggs Institute (JBI) checklist36 for randomized trials was utilized since all the studies were randomized trials37 (Appendix 1). The checklist contained 13 appraisal questions, but only applicable 10 questions were utilized. Articles are rated yes if they checked positive, no if they checked native, and unclear if they are unsure of whether they are positive or negative. At the end, overall ratings were based on %yes. Articles were considered high-quality if they scored 80% and above, moderate quality if they scored between 50% and 60%, and those below 50% were low quality and unfit for inclusion in this scoping review.
Noteworthy, following the appraisal of the eight included articles, it was interesting to note that all the studies were of high quality and had a low risk of bias, with none of the papers scoring less than 80% Yes (Table 1). Notably, Rodrigues et al38 was the only study that checked positive for all the checklist questions with 100%. True randomization, allocation concealment, and similarity at baseline were positive across all the studies. Similarly, there was a proper record of follow-up, measures, and reliability, and appropriate statistical analysis was considered by all the included studies.
 |
Table 1 Quality Assessment of the Included Studies
|
Data Extraction and Synthesis
Information pertinent to this review objective was synthesized into a formulated Excel form, allowing a summary of each article’s information under various headings. The information extracted includes the corresponding author name, year of publication, country, journal, aim of the paper, sample characteristics, ie, demographic data, settings, patients, design, virtual reality system used, description of the system, measures, instrument, method of data collection and analysis, result, and main findings (Appendix 2).
Moreover, the findings of the synthesis indicate that there has been a growing interest in the integration of virtual reality (VR) technology into breathing exercise program in recent years. As shown in Figure 2, there has been an increase in research in this domain.
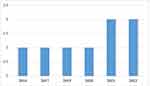 |
Figure 2 Article distribution by year.
|
The publications included in the study came from five distinct countries, with the United States and Brazil emerging as the major contributors. Each of these countries provided two articles, making them the most significant contributors among the eight papers analyzed. Similarly, the Journal of Applied Psychophysiology and Biofeedback exhibited the greatest quantity of publications, whereas the remaining articles were published in the Asian Journal of Nursing, Journal of Physical Medicine and Rehabilitation, Journal of Personalized Medicine, Journal of Applied Psychophysiology and Biofeedback, Journal of Medical Internet Research, and Journal of BMC Psychiatry.
Multiple convenient sample sizes were utilized, with an average sample size of 42 and a total sample size of 296. The sample population consists of individuals of both male and female genders, with a median age range spanning from 21.6 to 63.4 years. The individuals involved in the research were categorized as either in-patients or out-patients across the several investigations. The research involved patients or participants who shown a need to enhance their breathing functionality. All participants were randomly assigned to receive the VR-based intervention, and this assignment was conducted in accordance with relevant ethical consent procedures.
Narrative Synthesis
The study conducted by Kang et al39 in 2020 is the initial study included in the analysis, achieving a quality assessment score of 80%. The research utilized virtual reality technology to create an innovative breathing exercise solution that does not require contact with the mouth. Additionally, the study assessed the feasibility and effectiveness of this exercise technique. The proposed system is a virtual reality-based breathing exercise system, referred to as VR-BRES. The developers have integrated gaming features and a soft stretch sensor into their virtual reality-based self-regulatory biofeedback breathing workout system. The study assessed the feasibility and effectiveness of the system in comparison to the standard deep breathing (CDB) exercise. A total of 50 healthy participants (23 males and 27 females) with an average age of 42.52 ± 15.76 years were included in the analysis. The study involved individuals who were admitted as inpatients. Various respiratory parameters, such as forced vital capacity, forced expiratory volume in one second (FEV1), and peak expiratory flow (PEF), were assessed using a portable spirometry device called Pony FX (COSMED, USA). The utilization of the Virtual Reality-based Breathing Rehabilitation System (VR-BRES) yielded notable improvements in the parameters during the breathing rehabilitation program. Significantly, the outcomes of participants’ evaluations indicate that, in comparison to the standard deep breathing CDB exercise system, users regarded the breathing exercise with VR-BRES as more engaging, effective, and with a higher intention to utilize. Despite the lack of major differences in convenience across the various exercise approaches, However, the findings of the study indicate that virtual reality can serve as an effective training system for the purpose of respiratory rehabilitation.
Blum et al study20 assessed the feasibility of utilizing a virtual reality exercise system for diaphragmatic breathing with the incorporation of biofeedback algorithms. The VR-based system also employs a respiratory biofeedback method. To assess the effectiveness of this system, a total of 72 participants, with a majority of 56 females and 16 males, were randomly assigned to engage in a brief VR-based breathing exercise. The average age of the participants was 21.6 years. The study involved a group of outpatients, and the variables assessed included participants’ post-exercise experience, subjective breath awareness after exercising, respiratory-induced abdomen motions during the exercise, and heart rate variability throughout the exercise. These measurements were obtained using the Oculus Rift CV1. In comparison to a control group engaging in focused breathing exercises, the findings of the study suggest that a VR-based breathing exercise system, when integrated with biofeedback, enhances respiratory sinus arrhythmias with a particular emphasis on slow diaphragmatic breathing. Similarly, enhancing breathing awareness and achieving an elevated level of user satisfaction.
The study conducted by Betka et al40 focused on leveraging VR as a potential solution for addressing the issue of persistent dyspnea, often known as shortness of breath, among individuals in the recovery phase of COVID-19. The VR-based breathing workout system was utilized to construct a visual respiratory feedback function. The randomized experiment included a cohort of 26 participants, the majority of whom were male, with a median age of 55. The study involved individuals who were admitted as inpatients. The respiratory rate and respiratory rate variability were assessed as progression indicators of pulmonary rehabilitation. These parameters were recorded using the Go Direct® Respiration Belt, manufactured by Vernier, Beaverton, OR, USA. The intervention group was provided with synchronous feedback regarding their breathing, while the control group received asynchronous feedback. The assessment of the results was conducted using a combination of breathing recordings and questionnaires. The results of the trials suggest that the implementation of the Individual VR exercise system led to enhanced breathing comfort among participants in the intervention group, whereas no statistically significant improvements were observed in the control group. Although no negative effects were noted by the subjects, the research documented an increased level of user satisfaction and perception.
Cruz and collaborators conducted a study41 in which various parameters were measured, including blood pressure, heart rate, respiratory rate (RR), peripheral oxygen saturation (SpO2), and rating of perceived exertion (RPE). These measurements were obtained utilizing the Epson PowerLite H309A and Xbox One Kinect devices. However, the study discovered that virtual reality-based therapy (VRBT) significantly enhances breathing rehabilitation by influencing various physiological parameters such as heart rate, respiratory rate, and rate of perceived exertion. These effects were observed during the execution of VRBT as well as during moments of rest and at 1, 3, and 5 minutes of recovery. The present study involved a cluster trail done at an outpatient rehabilitation center in Brazil, with a sample of 27 individuals with a mean age of 63.4 years.
In a trial conducted by Ruzicky et al42 in which a pulmonary rehabilitation program, utilizing virtual reality technology to perform exercises, was provided to a group of 32 inpatient individuals diagnosed with COVID-19. The assessment included criteria such as breathing exercise tolerance and other factors. The findings from the trials indicate that the analysis of the initial data shown that a hospital-based pulmonary rehabilitation program lasting for a duration of three weeks resulted in enhanced exercise tolerance among those affected by COVID-19. Additionally, this program was associated with a decrease in symptoms related to depression and anxiety.
Rodrigues et al38 similarly examine the potential impact of VR on the experience of dyspnea, as well as other factors including pain symptom management, well-being perception, anxiety, and depression, in a sample of 44 hospitalized individuals with COVID-19. The average age of the participants is 48.9, and the distribution of samples is equal between genders. A novel biofeedback VR breathing exercise, incorporating gaming elements and a lens, was created for the purpose of assessing dyspnea as the major outcome. Additionally, the secondary outcomes of arterial hypertension, heart rate, respiratory rate, and SpO2 were also evaluated. Upon completion of the studies, it is evident that exercise therapy utilizing VR has a substantial impact on reducing symptoms of dyspnea as well as other measurable secondary outcomes.
A previous investigation conducted by Russell et al43 centered on the utilization of virtual reality to facilitate paced diaphragmatic breathing (DB) training. The study involved a randomized trial of 60 female outpatients who were assigned to receive a treatment consisting of VR-based breathing exercises. The study examined many outcomes, including heart rate variability, breathing rate, and assessments of motion nausea. It is important to note that heart rate variability is a controversial outcome measure herein. Heart rate variability is often used as an indicator of autonomic nervous system activity, specifically reflecting the balance between sympathetic and parasympathetic influences on heart rate. However, its interpretation as a direct measure of parasympathetic drive is subject to debate and caution. The study’s results indicate that the implementation of VR-based timed DB exercises leads to a notable enhancement in breathing functions and the activation of the parasympathetic nervous system (PNS). This activation of the PNS effectively mitigates physiological responses linked to motion sickness.
In a study conducted by Shiban et al,44 the researchers examined the use of diaphragmatic breathing as a coping strategy in the context of virtual reality exposure therapy for aviophobia. The trial comprised a cohort of 29 individuals, with a significant majority being female. The measurement of both heart rate and respiration rate was conducted after the VR-exposure treatment. The findings indicate that the incorporation of VR technology into diaphragmatic breathing exercises yields enhancements in respiratory functions and aids in the alleviation of aviophobia.
Discussion
This research presents a scoping review that investigates the significance of integrating virtual reality exercise into breathing rehabilitation. Although different breathing techniques like mindful breathing, focused breathing, diaphragmatic breathing, and abdominal breathing are commonly used in clinical settings, there is a growing interest in exploring how emerging virtual reality technology could help with slow and controlled breathing, which could help with relaxation and improve respiratory functions.
Based on the review of eight high-quality studies in this research, it is clear that VR technology has the potential to boost breathing function even more than traditional breathing exercises. This finding was corroborated by all of the trials included in the study. Of note, the majority of the reviewed papers relied on pilot studies or control studies as the basis for their research. Additionally, a subset of the papers focused solely on describing the design and development processes of their systems.
Blum et al20 showed that a VR-based tool can work and be useful for encouraging slow diaphragmatic breathing through biofeedback of the respiratory system. The research conducted involved the development of a VR system for conducting breathing exercises. The study revealed how well a respiratory biofeedback method used in virtual reality could teach people how to control their breathing patterns and improve their overall respiratory health. It was quite interesting that the VR system developed in their paper facilitates the regulation of participants’ respiration through the utilization of visual stimuli. Showing each participant, a virtual representation of their chest cavity, wherein the color of the cavity changed in accordance with the depth of their breath further enhance participant breathing awareness. Upon the conclusion of multiple virtual reality training sessions, the participants acquired the ability to regulate their breathing patterns in a consistent and profound manner. This, however, facilitate the acquisition of improved breathing management skills, as a result of the biofeedback on their respiratory patterns. The findings of this study proved the feasibility and acceptability of utilizing VR for breathing rehabilitation and respiratory biofeedback.
In contrast to different methods for breathing exercises, growing evidence and reports have consistently demonstrated the efficacy of the VR exercise system in enhancing breathing rehabilitation. This improvement is achieved through the utilization of the VR respiratory biofeedback technique, which not only offers participants an enjoyable and motivating experience but also provides them with valuable feedback on their breathing patterns. The observation of a notable rise in forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) after the VR-based breathing exercise training indicates the presence of this phenomenon. The integration of respiratory biofeedback techniques into the VR system in Blum study may presents a promising avenue for breathing rehabilitation, offering potential benefits offering potential benefits for individuals seeking to enhance their breathing capabilities. It was further underlined by the study that the advantages of VR can also be taken into account for several respiratory disorders, such as cystic fibrosis, COPD, and asthma, which may benefit from the technology.The link between success and the swift growth of VR breathing techniques may be attributed to the provision of a very engaging and immersive workout experience. All of the evaluated research consistently placed focus on these features. One of the studies,39 compared the efficacy and usefulness of a VR breathing exercise system to conventional deep breathing exercises. The findings of their trial indicated that although individual variations in breathing function exist, the use of a VR-based exercise system resulted in a noteworthy enhancement of breathing parameters. In-addition, their user reviews indicated that these training routines are highly captivating, enjoyable, and high intention to use.
Similar to Blum’s findings, the fact that biofeedback and self-regulation are part of the virtual reality exercise system may explain the success of the breathing exercise system. This finding aligns with assertions made by other scholars, as its distinctiveness correlates to the visualization of respiratory signals that offers respiratory feedback. This was also emphasized by Kang et al VR-based breathing exercise system,39 which provides biofeedback through breathing signal visualization, such as the avatar rabbit jump. The importance of this biofeedback was also underscored in a prior study, which demonstrated that women with limited thoracic movement experienced notable changes in respiratory parameters when incorporating visual feedback of diaphragmatic motion through ultrasound imaging into their VR breathing exercise regimen. Significantly, the transformation of the physical expansion of the chest or abdomen during inhalation into visual cues that are promptly relayed to the participants was effectively augment and engagement in breathing exercises was heightened.
The integration of bio-respiratory visual feedback into virtual reality exercise can also be utilized in addressing dyspnea38,40. In line with the findings of these authors, the inclusion of visual-respiratory feedback or self-regulating biofeedback in VR interventions may enhance the breathing comfort of patients in the recovery phase of COVID-19 pneumonia, particularly those who are experiencing persistent dyspnea. Betka et al further confirmed these through their clinical experiment, including patients who are undergoing recovery from COVID-19 and are persistently affected by dyspnea.40 The authors posited that in cases where alternative respiratory treatments or interventions prove ineffective and potentially result in serious complications such as cognitive impairments, mental health disorders, and motor impairments, the implementation of a virtual reality-based breathing exercise intervention could yield substantial success in addressing the issue of persistent dyspnea. This observation aligns with the findings of the Rodrigues et al study, wherein a significant decrease in dyspnea and fatigue was seen among those affected by COVID-19 following VR-based exercise intervention.38
Virtual reality breathing exercise intervention demonstrates a broader impact beyond its application to COVID-19 patients. This claim was similarly supported by a recent study which indicated that VR tool can also effectively reduce tiredness and dyspnea in obstructive pulmonary patients via administering virtual reality-based pulmonary rehabilitation.45
Additionally, a recent randomized control study conducted in Saudi Arabia (42) focused on children with repaired congenital diaphragmatic hernia (CDH), who are known to continue living with chronic lung issues and demonstrate lower cardiorespiratory fitness compared to their healthy counterparts. Consequently, there is a risk of declining functional performance and physical ability in these children due to reduced cardiopulmonary fitness. However, the study highlighted that when VR-based exercises are combined with traditional physical therapy, these children with repaired CDH experienced more significant improvements in their pulmonary functions, cardiopulmonary capacity, functional performance, and quality of life compared to those who received traditional physical therapy alone46. However, without a detailed explanation of the underlying mechanism of action, it is challenging to fully understand how VR-based exercises contribute to these positive outcomes. The absence of a conceptualized framework in several studies limits our ability to contextualize and interpret the study findings within a theoretical framework.
This growing evidence among adults and kids supports the assertion that a VR-based breathing exercise system can be considered as a potential alternative approach which is non-invasive and has no pharmacological features for promoting the rapid recuperation of patients.
This scoping review founds VR breathing exercise therapy to be a promising tool in terms of patient satisfaction and the potential to alleviate the breathing issues and persistent dyspnea commonly observed in individuals recovering from severe conditions like Covid-19. Clinical improvements were observed in various aspects as a result of the VR biofeedback breathing intervention. Participants demonstrated noteworthy improvements in fatigue levels, and overall comfort during breathing exercises. Moreover, positive alterations were observed in vital signs, encompassing heart rate and other cardiopulmonary parameters as reported by Betka et al.
To show how fast these rehabilitation techniques can be, limited exposure of people having breathing problems to short synchronous VR interventions incorporating visuo-respiratory features may improve breathing comfort. The uniqueness of the Immersive VR developed by Betka and associates and the VR-assisted therapeutic breathing exercise system developed by Rodrigues et al underscores the importance of cardiac or respiratory synchrony and self-regulating biofeedback.38,40 This synchrony creates a system that offers a better outcome. For example, the utilization of a “virtual body that is animated by the patient’s own respiratory movements”, a “complete duration of the breathing sequence”, and a comparable “three-dimensional virtual environment” contribute to enhanced involvement in breathing exercises.
The provision of synchronous feedback has been found to significantly enhance the perception of control among patients with respect to their respiratory function, as reported in multiple studies20,39,40. Consequently, this heightened sense of control contributes to the enhancement of breathing self-regulation and awareness. Although the initial stage of Betka’s study did not show a statistically significant decrease in breathing discomfort, it did reveal a notable improvement in overall breathing comfort when utilizing synchronous visuo-respiratory stimulation. The insignificant initial phase result may be attributed to semantics or subjective discomfort ratings. This claim is consistent with the findings of a study conducted recently on the effects of a virtual reality-based breathing therapy on physiological responses in breathing rehabilitation.41 Specifically, their findings indicated that this therapy is effective in conditioning the participants during the execution phase. However, it was noted that elevated levels of respiratory rate and other cardiac parameters may be achieved during the recovery phase, and these effects can persist for up to 5 minutes. It is not surprising that such interventions can have an impact on various hemodynamic functions during the recovery phase, even up to a few minutes after the activity has ended. Nevertheless, the diverse effects observed in their virtual reality breathing therapy may be attributed to the differential levels of effort and intensity applied during the treatment. These, however, raise the importance of exercising caution throughout the administration of the virtual reality intervention, particularly in terms of closely monitoring the level of virtual reality exertion.
Betka40 and Cruz41 successfully demonstrated the safety and cost-effectiveness of immersive VR-based digital therapeutics and virtual reality breathing therapy. They posited that VR-based interventions can be utilized as alternative cardiovascular interventions for individuals who are either in-patients or out-patients and are facing respiratory or breathing challenges. This tool can offer a supplementary approach for treatment and assessment, thereby reducing the potential for transmission and mitigating the established adverse effects linked to opioid therapy.
Additionally, this scoping review identified exercise tolerance; a key indicator of cardiovascular endurance during breathing rehabilitation, and the implications of optimal lung function as another important area in which VR can be leveraged. This was supported by Ruzicky et al investigation on the importance of VR in enhancing exercise tolerance.42 They emphasize incorporation of VR-breathing exercise rehabilitation into COVID-19 rehabilitation therapy due to its numerous advantages in enhancing respiratory problems. Their three-week VR pulmonary rehabilitation program for COVID-19 inpatients demonstrated a noteworthy effect, as patients exhibited notable improvements in exercise tolerance subsequent to exposure to VR breathing exercise. While there was a gain in functional ability, the improvement in quality of life was not found to be significant, and no notable advantage over conventional treatments was noted. This observation is in contrast with the conclusions drawn by previous researchers, who discovered a notable and distinct advantage of VR breathing exercises over traditional rehabilitation interventions.
The preliminary nature of the data analysis in the their study42 and brief duration of the VR exposure may be attributed to the insignificance findings. Therefore, possibly conducting a re-evaluation with a more extensive sample size over long period of exposure could potentially yield a positive outcome. Despite these findings, the author asserts, in alignment with prior research, that the integration of VR into breathing rehabilitation therapy presents a viable approach for mitigating the long-term consequences of COVID-19 and other respiratory ailments.
This review synthesizes evidence suggesting that VR breathing exercise interventions have the potential to yield more favorable outcomes compared to conventional interventions. Specifically, these interventions can effectively promote increased awareness of patients’ breathing status and facilitate the maintenance of a balanced pulmonary function. Moreover, VR exercise tool’s ability to provide entertainment, engagement, and interactivity aligns with its distinct advantage over usual exercise methods that entail passive exercise participation. This, however, leads users to see exercise, typically seen as a highly demanding activity, as an enjoyable and immersive experience owing to its interactive characteristics.
In comparison to traditional breathing exercise interventions, a study conducted by Russell et al demonstrated that the diaphragmatic breathing protocol resulted in a drop-in respiration rate, an increase in parasympathetic nervous system tone, and a reduction in the occurrence of motion sickness symptoms.43 The objective of activating the parasympathetic nervous system, as indicated by an increase in heart rate variability, was successfully accomplished, potentially resulting in the prevention of symptoms associated with motion sickness. Furthermore, these findings provide additional support for the assertion that the utilization of VR breathing exercises might effectively mitigate the progression of symptoms associated with motion sickness resulting from breathing control. The confluence of diaphragmatic breathing mechanisms and reduced respiratory rate suggests that these methods have the potential to enhance parasympathetic tone and provide a safeguard against motion sickness when individuals are exposed to stimuli that induce motion sickness. Despite concerns regarding potential risks associated with diaphragmatic breathing exposure during VR exercise therapy, evidence suggests that diaphragmatic breathing during VR intervention does not moderate negative outcomes.44 On the contrary, it has been found to enhance the effectiveness of VR breathing exercise rehabilitation and alleviate conditions such as aviophobia, which involves a fear of flying.
Considering the long-term effects is crucial for understanding the true potential and effectiveness of VR-based exercise interventions in the context of respiratory conditions. Future studies should address this limitation by incorporating follow-up evaluations to provide a more comprehensive understanding of the treatment’s lasting impact.
Limitation and Conclusion
Limitation
The heterogeneous nature of the VR system and the biofeedback mechanisms and techniques employed by the different included studies may be considered the main limitations of this scoping review. Since the primary objective of each respective study varies, the outcome may vary with studies. Limited numbers of trials may also be a potential limitation, as it is difficult to conclude with limited evidence. Nonetheless, the scoping review of eight quality studies in these current papers confirmed the significance of taking advantage of VR in breathing exercise rehabilitation.
It is noteworthy that the findings of some reported studies exhibit variability due to factors such as constraints in experimental design methodology, inadequate availability of objective measurable breathing outcomes, and limited sample sizes. We encourage readers to conduct a more critical appraisal of the article/topic(s) of interest to form an independent and informed judgment regarding the effectiveness and implications of breath training with/without the VR in the context of their specific clinical population.
Conclusion
The effectiveness and rapid growth of VR breathing techniques are attributed to their engaging and immersive experience. The integration of biofeedback and self-regulation in VR exercise systems was also found to contribute to the significant outcome of the breathing exercise system. This is because the use of visual feedback in VR breathing exercises enhances user interest in breathing exercises.
In addition, this scoping review highlights the effectiveness of VR exercise in improving dyspnea, a breathing condition. The unique aspect of VR-assisted breathing exercise systems lies in their emphasis on cardiac or respiratory synchrony and self-regulating biofeedback. The inclusion of a “virtual body animated by the patient’s own breathing” and a 3D virtual environment enhances engagement, self-regulation, and awareness during breathing exercises. However, the review also indicates that the outcomes of VR rehabilitation can vary depending on the effort and intensity exerted. Therefore, careful monitoring of VR effort intensity is necessary. Overall, VR breathing exercises are considered safe and cost-friendly rehabilitation tools for both in-patients and out-patients with respiratory difficulties.
Additionally, the paper suggests that VR breathing exercise interventions offer preventive measures against the prolonged effects of conditions such as COVID-19 and other respiratory conditions. These interventions motivate patients to be mindful of their breathing condition and maintain balanced pulmonary function. The entertaining, engaging, and interactive nature of VR exercise therapy adds a fun and immersive element to the overall exercise experience for users.
Abbreviations
COPD, chronic obstructive pulmonary disease; CDH, congenital diaphragmatic hernia; DB, diaphragmatic breathing; FEV1, forced expiratory volume in one second; HIIT, high-intensity interval training; JBI, Jonna Briggs Institute; VR, virtual reality; VRBT, virtual reality-based therapy; PNS, parasympathetic nervous system; PR, Pulmonary rehabilitation.
Acknowledgments
The author would like to thank the College of Applied Medical Sciences Research Center and the Deanship of Scientific Research at King Saud University.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Pleil JD, Ariel Geer Wallace M, Davis MD, Matty CM. The physics of human breathing: flow, timing, volume, and pressure parameters for normal, on-demand, and ventilator respiration. J Breath Res. 2021;15(4):042002. doi:10.1088/1752-7163/ac2589
2. Nelson N. Diaphragmatic breathing: the foundation of core stability. Strength Conditioning J. 2012;34(5):34–40. doi:10.1519/SSC.0b013e31826ddc07
3. Pawaria S. Breathing- mechanism of breathing, muscles of respiration, breathing pattern and breathing exercises. In: DrTM A, editor. Emerging Trends in Disease and Health Research Vol. 6. Book Publisher International (a Part of SCIENCEDOMAIN International). 2022:128–141. doi:10.9734/bpi/etdhr/v6/15350D
4. Lu HB, Ma RC, Yin YY, Song CY, Yang TT, Xie J. Clinical indicators of effects of yoga breathing exercises on patients with lung cancer after surgical resection: a randomized controlled trial. Cancer Nurs. 2023. doi:10.1097/NCC.0000000000001208
5. Kader M, Hossain M, Reddy V, Perera NKP, Rashid M. Effects of short-term breathing exercises on respiratory recovery in patients with COVID-19: a quasi-experimental study. BMC Sports Sci Med Rehabil. 2022;14(1):60. doi:10.1186/s13102-022-00451-z
6. Gerage AM, Alberton CL, Cucato GG, Delevatti RS, Ritti-Dias RM. Editorial: exercise intervention for prevention and management of hypertension. Front Physiol. 2023;14:1244715. doi:10.3389/fphys.2023.1244715
7. Hopper SI, Murray SL, Ferrara LR, Singleton JK. Effectiveness of diaphragmatic breathing for reducing physiological and psychological stress in adults: a quantitative systematic review. JBI Database Syst Rev Implement Rep. 2019;17(9):1855–1876. doi:10.11124/JBISRIR-2017-003848
8. Cai Y, Ren X, Wang J, Ma B, Chen O. Effects of breathing exercises in patients with chronic obstructive pulmonary disease: a network meta-analysis. Arch Phys Med Rehabil. 2023;S0003999323002836. doi:10.1016/j.apmr.2023.04.014
9. Martins A, Arienzo A. Experiences and preferences of persons with asthma regarding breathing exercises are more related to wellness than to healthcare. Pneumologie. 2023;77(S 01):Po–436. doi:10.1055/s-0043-1761127
10. Hussein EE, Taha NM. Effect of breathing exercises on quality of recovery among postoperative patients. Int J Stud Nurs. 2018;3(3):151. doi:10.20849/ijsn.v3i3.525
11. Gholamrezaei A, Van Diest I, Aziz Q, Vlaeyen JWS, Van Oudenhove L. Psychophysiological responses to various slow, deep breathing techniques. Psychophysiology. 2021;58(2):e13712. doi:10.1111/psyp.13712
12. Apriliana D, Suradi S, Setijadi AR. Role of incentive spirometry on exercise capacity, breathing symptoms, depression rate, and quality of life in NSCLC patients with chemotherapy. Respir Sci. 2021;2(1):8–17. doi:10.36497/respirsci.v2i1.33
13. Suharti A, Rachmawati Nur Hidayati E, Yusviani HA. Comparative effect of incentive spirometry and diaphragm breathing to functional capacity in COVID-19 patient in an isolated ward. Bali Med J. 2022;11(3):1415–1419. doi:10.15562/bmj.v11i3.3579
14. Wang YQ, Cao HP, Liu X, et al. Effect of breathing exercises in patients with non-small cell lung cancer receiving surgical treatment: a randomized controlled trial. Eur J Integr Med. 2020;38:101175. doi:10.1016/j.eujim.2020.101175
15. Arden-Close E, Teasdale E, Tonkin-Crine S, et al. Patients’ perceptions of the potential of breathing training for asthma: a qualitative study. Prim Care Respir J. 2013;22(4):449–453. doi:10.4104/pcrj.2013.00092
16. Morrow B, Brink J, Grace S, Pritchard L, Lupton-Smith A. The effect of positioning and diaphragmatic breathing exercises on respiratory muscle activity in people with chronic obstructive pulmonary disease. South Afr J Physiother. 2016;72(1):6. doi:10.4102/sajp.v72i1.315
17. Lee K, Choo Y-KI. Inspiratory muscle strengthening training method to improve respiratory function: comparison of the effects of diaphragmatic breathing with upper arm exercise and power-breathe breathing. J Korean Soc Integr Med. 2021;9(3):201–211. doi:10.32625/KJEI.2021.24.201
18. Yang Y, Wei L, Wang S, et al. The effects of pursed lip breathing combined with diaphragmatic breathing on pulmonary function and exercise capacity in patients with COPD: a systematic review and meta-analysis. Physiother Theory Pract. 2022;38(7):847–857. doi:10.1080/09593985.2020.1805834
19. Kotta PA, Ali JM. Incentive spirometry for prevention of postoperative pulmonary complications after thoracic surgery. Respir Care. 2021;66(2):327–333. doi:10.4187/respcare.07972
20. Blum J, Rockstroh C, Göritz AS. Development and pilot test of a virtual reality respiratory biofeedback approach. Appl Psychophysiol Biofeedback. 2020;45(3):153–163. doi:10.1007/s10484-020-09468-x
21. Kouijzer MMTE, Kip H, Bouman YHA, Kelders SM. Implementation of virtual reality in healthcare: a scoping review on the implementation process of virtual reality in various healthcare settings. Implement Sci Commun. 2023;4(1):67. doi:10.1186/s43058-023-00442-2
22. Miner N. Stairway to Heaven: Breathing Mindfulness into Virtual Reality. Northeastern University; 2022. doi:10.17760/D20471083
23. Li S, Zheng H, Ge Y, Yuan W, Han T Designing mindfulness practice system based on biofeedback in VR environment. In: Volume 2: 42nd Computers and Information in Engineering Conference (CIE). American Society of Mechanical Engineers; 2022:V002T02A090. doi:10.1115/DETC2022-91254.
24. Subramanian SK. Virtual reality in rehabilitation—using technology to enhance function. Pm&r. 2018;10(11):1221–1222. doi:10.1016/j.pmrj.2018.11.001
25. Li BJ, Peña J, Jung Y. Editorial: VR/AR and wellbeing: the use of immersive technologies in promoting health outcomes. Front Virtual Real. 2023;3:1119919. doi:10.3389/frvir.2022.1119919
26. Dar S, Ekart A, Bernardet U The virtual human breathing coach. In: 2022 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW). IEEE; 2022:434–436. doi:10.1109/VRW55335.2022.00095.
27. Freeman D, Reeve S, Robinson A, et al. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol Med. 2017;47(14):2393–2400. doi:10.1017/S003329171700040X
28. Pancini E, Anna FDN, Villani D. Breathing in virtual reality for promoting mental health: a scoping review. Preprint. 2023;1–43.
29. Hoeg ER, Bruun-Pedersen JR, Serafin S Virtual reality-based high-intensity interval training for pulmonary rehabilitation: a feasibility and acceptability study. In: 2021 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW). IEEE; 2021:242–249. doi:10.1109/VRW52623.2021.00052.
30. Cook NE, Huebschmann NA, Iverson GL. Safety and tolerability of an innovative virtual reality-based deep breathing exercise in concussion rehabilitation: a pilot study. Dev Neuro Rehabil. 2021;24(4):222–229. doi:10.1080/17518423.2020.1839981
31. Snyder A, Sheridan C, Tanner A, et al. Cardiorespiratory functioning in youth with persistent post-concussion symptoms: a pilot study. J Clin Med. 2021;10(4):561. doi:10.3390/jcm10040561
32. Condon C, Lam WT, Mosley C, Gough S. A systematic review and meta-analysis of the effectiveness of virtual reality as an exercise intervention for individuals with a respiratory condition. Adv Simul. 2020;5(1):33. doi:10.1186/s41077-020-00151-z
33. Lan KC, Li CW, Cheung Y. Slow breathing exercise with multimodal virtual reality: a feasibility study. Sensors. 2021;21(16):5462. doi:10.3390/s21165462
34. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
35. Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Health. 2015;13(3):141–146. doi:10.1097/XEB.0000000000000050
36. Barker TH, Stone JC, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid Synth. 2023;21(3):494–506. doi:10.11124/JBIES-22-00430
37. Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L. Chapter 3: systematic reviews of effectiveness. JBI Manual for Evidence Synthesis. 2020;3. doi:10.46658/JBIMES-20-04
38. Rodrigues IM, Lima AG, Santos AED, et al. A single session of virtual reality improved tiredness, shortness of breath, anxiety, depression and well-being in hospitalized individuals with COVID-19: a randomized clinical trial. J Pers Med. 2022;12(5):829. doi:10.3390/jpm12050829
39. Kang J, Hong J, Lee YH. Development and feasibility test of a mouth contactless breathing exercise solution using virtual reality: a randomized crossover trial. Asian Nurs Res. 2021;15(5):345–352. doi:10.1016/j.anr.2021.12.002
40. Betka S, Kannape OA, Fasola J, et al. Virtual reality intervention alleviates dyspnoea in patients recovering from COVID-19 pneumonia. ERJ Open Res. 2023;9(6):00570–02022. doi:10.1183/23120541.00570-2022
41. Alves Da Cruz MM, Ricci-Vitor AL, Bonini Borges GL, Fernanda Da Silva P, Ribeiro F, Marques Vanderlei LC. Acute hemodynamic effects of virtual reality–based therapy in patients of cardiovascular rehabilitation: a cluster randomized crossover trial. Arch Phys Med Rehabil. 2020;101(4):642–649. doi:10.1016/j.apmr.2019.12.006
42. Ruzicky E, Sramka M, Sramka M, et al. Providing prevention, diagnosis, and treatment of patients after COVID-19 using artificial intelligence. Neuro Endocrinol Lett. 2022;43(1):9–17.
43. Russell MEB, Hoffman B, Stromberg S, Carlson CR. Use of controlled diaphragmatic breathing for the management of motion sickness in a virtual reality environment. Appl Psychophysiol Biofeedback. 2014;39(3–4):269–277. doi:10.1007/s10484-014-9265-6
44. Shiban Y, Diemer J, Müller J, Brütting-Schick J, Pauli P, Mühlberger A. Diaphragmatic breathing during virtual reality exposure therapy for aviophobia: functional coping strategy or avoidance behavior? A pilot study. BMC Psychiatry. 2017;17(1):29. doi:10.1186/s12888-016-1181-2
45. Jung T, Moorhouse N, Shi X, Amin MF. A virtual reality–supported intervention for pulmonary rehabilitation of patients with chronic obstructive pulmonary disease: mixed methods study. J Med Internet Res. 2020;22(7):e14178. doi:10.2196/14178
46. Azab AR, Elnaggar RK, Abdelbasset WK, et al. Virtual reality-based exercises’ effects on pulmonary functions, cardiopulmonary capacity, functional performance, and quality of life in children with repaired congenital diaphragmatic hernia. Eur Rev Med Pharmacol Sci. 2023;27(14):6480–6488. doi:10.26355/eurrev_202307_33118


")