
The primary function of breathing is to absorb oxygen from the air and to get rid of the waste – carbon dioxide – via the movement of the lungs.
When there is a narrowing in the airways (stenosis) that obstructs the passage of air into the lungs, it can affect the larynx, trachea and surrounding structures.
Without enough air, breathing and speech are disrupted, and you may experience shortness of breath or chest tightness.
Often, it could be a symptom of heart and lung problems, or other conditions such as asthma, allergies or anxiety.
In the past, there was no way to treat airway stenosis, but now there is hope with interventional pulmonology (IP), a subspeciality of respiratory medicine.
Using a scope
IP uses minimally-invasive techniques to diagnose and treat lung cancer, pleural diseases (which affect the thin layers of tissue that protect the lungs), and many types of complex airway and lung disorders.
The technique is similar to a coronary angioplasty procedure, where balloons are placed to stretch and widen a narrowed artery.
“Here, we dilate the airway to make it bigger, and sometimes, we also put in stents, although the material used is different from the cardiac stents.
“Airway stents are most commonly made of silicon,” says Dr Jamalul Azizi Abdul Rahaman, a consultant pulmonologist (respiratory physician) at Hospital Idris Shah, Serdang, Selangor (formerly known as Hospital Serdang).
“Before IP was introduced in Malaysia, we had to send our patients (with airway stenosis) to Singapore for treatment as we didn’t have the expertise available in our country.
“If patients couldn’t afford it, they simply had to suffer.
“We couldn’t do anything except to pray for the best as there are no medicines that can relieve the narrowing.”
Most IP procedures involve some form of bronchoscopy, which enables minimally-invasive interventions using tiny cameras or surgical tools passed through a thin bendable tube called a bronchoscope.
It’s inserted through the nose or mouth, into the lungs.
The bronchoscope enables the doctor to:
- Look for and treat tumours, bleeding, inflammation or blockages in the lungs or airways
- Obtain fluid samples or tissue biopsies for testing
- Dilate narrowed areas, and
- Implant stents.
And all this can be done without the patient having to undergo surgery or hospitalisation as it is usually a daycare procedure.
First line of treatment
Dr Jamalul explains: “We can also do interventions for asthma and chronic obstructive pulmonary disease (COPD) cases. This patient has severe stenosis, or narrowing, in one of their airways due to tuberculosis. — Photos: Dr JAMALUL AZIZI ABDUL RAHAMAN
This patient has severe stenosis, or narrowing, in one of their airways due to tuberculosis. — Photos: Dr JAMALUL AZIZI ABDUL RAHAMAN
“For someone with emphysema, we can reduce the lung volume and make the patient breathe better.”
He shares: “Some of the implants can be left inside for many years.
“I had a patient with COPD, and the lungs were really inflated.
“So we put an endobronchial valve in and it has been there for more than eight years now – the patient is still doing fine.”
Endobronchial valves are removable, one-way valves that reduce lung hyperinflation by allowing the trapped air to escape.
As a result, lung function may improve as healthier areas of the lungs provide the necessary oxygen exchange.
Since these valves were introduced here a decade ago, Dr Jamalul has implanted them on 35 patients – all with great success.
For patients with tumours obstructing the airway, IP has made removing such tumours much easier.
“They’re suffocated with a big tumour and the only way is to take it out.
“Before, the thoracic surgeon would have to cut them up to remove the tumour, or even to do a biopsy, but now, these patients don’t need major surgery.
“We remove a chunk and fire the remaining bits with a laser to flatten the area,” he says.
However, Dr Jamalul points out that not every case will have a good outcome.
“In a small percentage of patients, we’re still unable to remove the tumour completely; then we have to refer them to the surgeon,” he says.
Basically, when a patient comes in with breathing difficulty, they will be assessed and referred to a lung specialist.
The specialist will then take the patient’s history and order a chest X-ray or lung CT (computed tomography) scan.
If intervention is necessary, the IP option is given, and if that fails, the patient is referred to the thoracic surgeon.
“If I get a diagnosis with IP, then it’s great, but if not, the second step will require the surgeon to cut and see where the problem lies.
“We’re not competing with the surgeon, but working with them.
“For cancer patients, they need a multidisciplinary team comprising an interventional pulmonologist or lung physician, cardiothoracic or thoracic surgeon, oncologist, and if necessary, a radiologist,” he explains.
First to be trained
Dr Jamalul, who is the chairman of the Malaysian Association for Bronchology & Interventional Pulmonology, was the first lung physician to undergo IP training in France in 2007.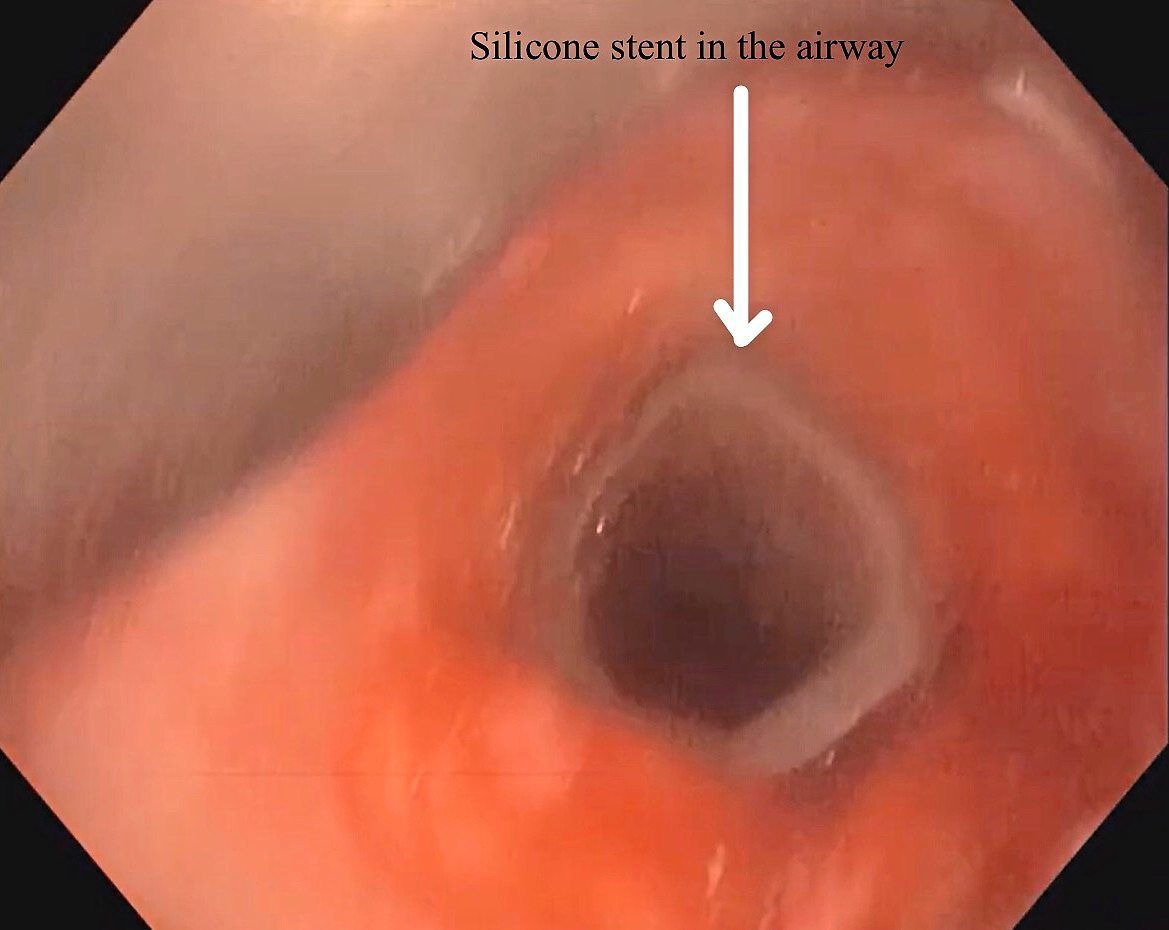 Here's a silicon stent that has been inserted to widen the airway.
Here's a silicon stent that has been inserted to widen the airway.
Subsequently, more respiratory specialists have followed suit.
At present, Malaysia has around 30 to 40 interventional pulmonologists, although only a handful, such as Dr Jamalul, have achieved the highest level of certification.
He says: “Almost every lung specialist nowadays can perform level one procedures, but maybe only about 10 can do level five, which is the most advanced.”
Other public hospitals offering IP services are Sarawak General Hospital in Kuching, Sarawak; Queen Elizabeth Hospital in Kota Kinabalu, Sabah; and Sultanah Bahiyah Hospital in Alor Setar, Kedah.
Unfortunately, despite all the advances in medical technology, IP cannot help patients with pulmonary fibrosis (lung scarring).
This is a group of interstitial lung diseases where the lungs become progressively stiffer and smaller, eventually leading to low oxygen levels in the blood and breathing difficulty.
Scars on the lung tissue can cause it to thicken and lose elasticity.
This can occur due to certain health conditions, medical treatment or exposure to hazardous materials.
In most cases, doctors can’t pinpoint what is causing the problem; however, post-Covid-19, Dr Jamalul shares that he is seeing more cases of pulmonary fibrosis.
He says: “This is especially the case in those who were ventilated for long periods – they get complications such as airway stenosis.
“People think putting a tube inside to ventilate is not a problem.
“It may save the life, but if the patient has been on prolonged intervention for more than two weeks, they might get something called post-intubation tracheal stenosis or ventilator-associated pneumonia.
“Not many people are aware of this potentially severe condition.”
The lung damage caused by pulmonary fibrosis cannot be repaired, but medications and therapies can sometimes help ease symptoms and improve quality of life.
“We can only offer them IP to make a diagnosis.
“The only treatment if the scarring is severe is a lung transplant,” he says.
Soon to come
The increase in the number of advanced tools used in IP has enabled a more accurate diagnosis of lung cancer.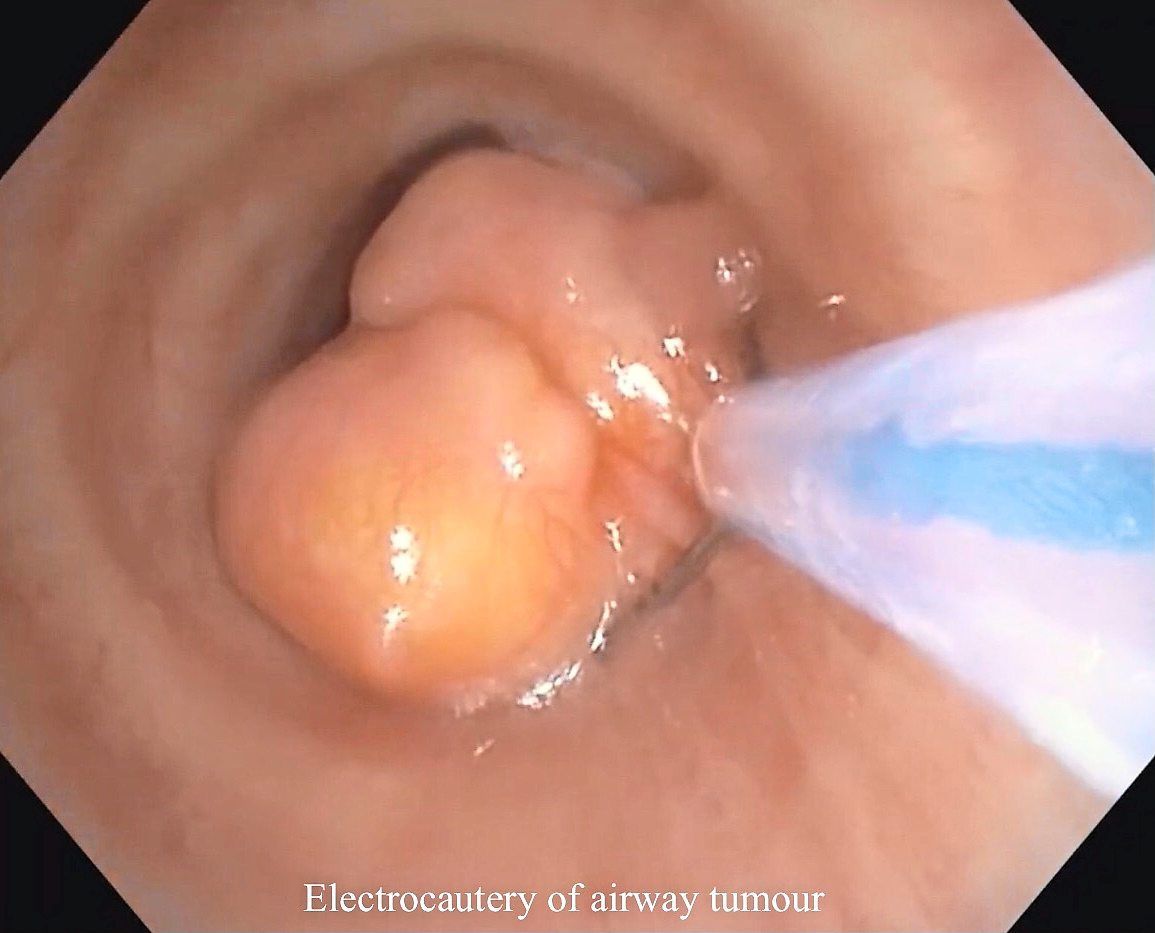 These large tumours that obstruct the airway can mostly be removed with IP.
These large tumours that obstruct the airway can mostly be removed with IP.
He shares: “For example, with robotic bronchoscopy, we can go into a very remote area of the lung and find the smallest cancer spot.
“However, this technology is not available in Malaysia yet, although it’s being used in the United States, Europe and Hong Kong.
“Apart from robotics, almost every IP procedure can be performed here, and patients don’t have to go elsewhere to seek treatment.”
In fact, for patients with lung cancer, chemotherapy can also be administered directly to the tumour cell using IP, so patients can avoid the systemic side effects that affect the whole body.
“We are going to start the service (called bronchoscopic intra-tumoral injection) soon in Serdang and we’ll be the first hospital in Malaysia to do so.
“We’re inviting an expert from Taiwan to guide us on the procedure,” says Dr Jamalul, who is excited to be part of the pioneering team in Malaysia to offer this new service to lung cancer patients.

















