
Chronic obstructive pulmonary disease (COPD), as the name implies, is a chronic lung disorder that restricts the outflow of air leading to breathing difficulties. It is a debilitating disease that gradually reduces the quality of life if not managed properly. It includes two subtypes namely; emphysema and chronic bronchitis.
COPD Symptoms
Emphysema involves abnormal enlargement of the alveolar sacs followed by permanent damage of the lining. This leads to reduced gaseous exchange and increased air trapping. Chronic bronchitis involves long-term inflammation of the lungs leading to irritation and breathing difficulties. Both conditions lead to airway obstruction, breathing difficulties, and chronic cough.
Read Also: Spirometry Doesn’t Fully Reveal Tobacco-Induced Lung Damage, Study Finds
It is worth noting that in 2019, 3.23 million people died from COPD, making it the third most common cause of death globally. Measured using disability-adjusted life years (DALY), COPD is the 7th most common cause of ill health worldwide. People with COPD are becoming more widespread throughout the world. Increased smoking rates worldwide and exposure to pollutants found in biomass fuels like wood and grass are two important factors that contribute to COPD.
Interestingly, the death rate of people with COPD has risen due to the COVID-19 pandemic that ravaged the world. Being hospitalized or passing away from COVID-19 was more likely in people with COPD due to their already compromised airways. Nevertheless, the pandemic saw fewer hospitalizations of COPD patients than it had in the past due to increased utilization of personal protective equipment and self-awareness.
There is no cure for COPD, however, the management protocols are diverse and could improve symptoms for patients who are willing to adhere to them.
Table of Contents
Causes of COPD
Airway obstruction in COPD is caused by clogging of the airways with mucus, inflammation, and swelling of the bronchial lining. All these lead to narrow airways and difficulty in breathing.
The single most important risk factor in the development of COPD is tobacco smoking. This involves exposure by active or passive means.
According to studies, smoking accounts for 8 out of 10 COPD-related deaths. COPD affects 15% of smokers on average. Smokers experience a faster decline in lung function as they age compared to non-smokers. If people stop smoking, their lungs work better.
Smoke exposure from the combustion of biomass and fossil fuels predisposes individuals to COPD. This is greatly seen in low and middle-income countries.
A person could also be at risk for developing COPD due to genetic factors. Alpha-1 antitrypsin deficiency is a rare genetic condition in which there is insufficient production of alpha-1 antitrypsin. This protein prevents neutrophil elastase from destroying lung tissue. Unfortunately, people with this deficiency develop emphysema by early middle age. This risk of developing emphysema in these groups of individuals is increased by smoking.
Respiratory problems at birth and in childhood slow lung growth and this could lead to COPD later in life. Also, people with asthma are likely to come down with the disease too.

Lung Tissue With COPD
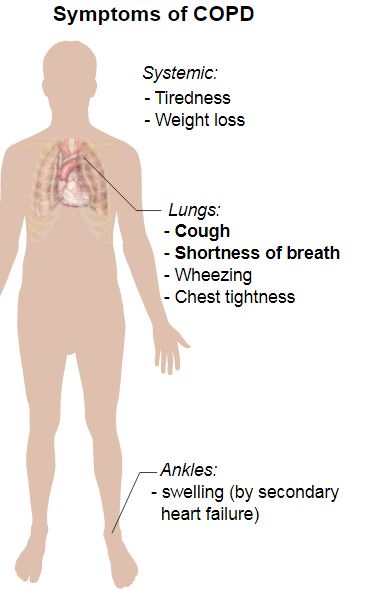
Symptoms
The clinical history of COPD is slow and progressive. There is an early phase and a late phase. The most common symptoms are chronic cough, difficulty in breathing, and exhaustion.
There may or may not be sputum production following the cough and it is usually worse on waking up. The shortness of breath usually happens during exertion. This may be attributed to lack of exercise or aging and dismissed in the process.
Sometimes breathing difficulties could also follow a lung infection because people with COPD are prone to frequent lung infections. As the disease progresses, it becomes more difficult to carry out normal daily activities.
It is said that about a third of patients with severe COPD may complain of weight loss. There is no known reason for weight loss, and different people may experience different causes. The inability to eat properly due to breathing difficulty is a possible factor.
COPD flare-up
Sometimes, the symptoms could be exacerbated leading to worsening cough, sputum production, and breathing difficulty. All these could happen when the person is at rest, especially breathing difficulty, leading to hospitalization. The color of sputum at this time changes to yellow or green.
This could lead to a life-threatening condition known as acute respiratory failure. Contributory symptoms include cyanosis, sweating, and confusion. Triggering factors are allergens like dust and fumes, and bacterial or viral infections.
Diagnosis
COPD is diagnosed based on a history of prolonged productive cough and breathing difficulty. Also, a thorough physical examination and laboratory tests are required. However, sometimes patients present late with advanced lung disease.
On examination, in mild cases, doctors may elicit nothing. As the condition worsens, wheezing and decreased breath sounds might become evident on listening to the lungs with a stethoscope. During breathing, the chest moves less and they might breathe by using their neck and shoulders.
Chest X-rays or computed tomography (CT) scans are useful in lung assessment. In mild forms of the disease, the film is usually normal and doesn’t show much but as the disease progresses, inflation of the lungs may be visible.
Spirometry is the primary COPD test. It is a type of lung function test that can diagnose COPD before the appearance of symptoms. It measures the amount of air a person exhales (known as forced expiratory volume, FEV) in one breathing cycle. Additionally, it gauges how quickly a person can expel air. The FEV in 1 second (FEV1) decreases in COPD patients.
A professional gives instructions to blow forcefully into a tube that is attached to a little machine. The device is known as a spirometer.
Also, an oxygen saturation test is very important. This is done by telling the patient to place a finger in a portable machine called a pulse oximeter or by collecting a blood sample for arterial blood gas analysis. The values are interpreted following these procedures. In persons with COPD, oxygen levels are frequently low. Late in the course of the disease, high quantities of carbon dioxide are found in the arteries.
Read Also: New Hope for COPD Patients: Early Trials Show Promise in Lung Cell Transplants
For younger people with alpha-1 antitrypsin deficiency, the level in the blood is analyzed. COPD is suspected in youngsters who have never smoked.
Other tests include electrocardiography and echocardiography to exclude heart disease. Heart disease is a prominent cause of breathing difficulties.
Treatment
The efficacy of COPD treatment is made possible by patient-doctor cooperation. Treatment of this condition involves lifestyle modification and drug therapy, all to improve symptoms.
The most important factor in lifestyle modification to consider is smoking cessation. When COPD patients quit smoking, symptoms considerably improve and the medications work better.
Strategies to stop smoking include; committing to a specific date for smoking cessation, increase in smoking intervals, making cigarettes hard to obtain, and using nicotine patches, gums, or inhalers.
Airways irritants should be avoided including passive smoking and air impurities. This could also involve relocation from an air-polluted area to an area with clean air.
Prompt treatment of lung infections is also beneficial. Infections like influenza and pneumonia could worsen disease conditions, therefore all COPD patients should get vaccinated against these infections including against COVID-19.
Lifestyle modification also involves a healthy balanced diet and nutritious foods, since COPD causes weight loss.
Drug treatment includes anticholinergic drugs like ipratropium, tiotropium, aclidinium, and revefenacin; short-acting beta-adrenergic (SABA) agents like albuterol and long-acting beta-adrenergic (LABA) agents like salmeterol and formoterol. Anticholinergic and beta-adrenergic drugs come in combinations like glycopyrrolate.
These drugs can be administered through a metered dose inhaler with or without a spacer device, and a nebulizer in emergencies.
Oxygen therapy might be required by some people with severe conditions including flare-ups. Oxygen tanks and oxygen concentrates are used to deliver it.
Read Also: Delivering Antibiotics with the Help of Microrobots Highly Effective in Treating Deadly Pneumonia
In severe cases of severe airway obstruction in younger patients, lung transplantation is often recommended. This improves quality of life.
Complications
Complications may develop if low oxygen levels are not corrected with supplementary oxygen. They include secondary polycythemia, leg swelling, heart rhythm abnormalities, pulmonary hypertension, heart failure, osteoporosis, depression, and coronary artery disease.
Current trends in COPD management
As the burden of COPD rises, healthcare professionals continually look for new ways to manage the disease. Digital health has been acknowledged as a potential remedy to lessen the load and enhance COPD care on a large scale.
Therefore, electronic health records, digital healthcare systems, telemedicine applications, and other applications that use digital technologies for health are all included in the term “digital health” in a broad sense.
These involve remote monitoring of symptoms by healthcare providers, face-to-face real-time video meetings, and remote consultation via email and smartphone direct messages.
Clinical Opinions
Smoking cessation is forefront and first-line in the management of COPD with the aim of conserving existing lung function. However, due to the background neurochemistry involved in the formation of habits, it can be close to impossible to quit smoking. Weeks spent smoke-free can be almost immediately followed by months of relapse. In my experience, a very effective way of stopping smoking for good is letting people around you that you respect know that you no longer smoke. Say it often, and slowly you will create an identity for yourself as a non-smoker (or at least an aspiring one).
This maneuver if skillfully carried out will lead to a position where your mind begins to associate smoking with a loss of respect, especially from people who you desire that they respect you. Once this position is reached, half the struggle is done and the rest is reinforcement. It can be a very shameful process, but if it leads to you having more years when you can breathe properly, it’s absolutely worth it.
Read Also: Organ Transplantation: Researchers Change Blood Type A Donor Lungs to Universal Type O Blood Lungs
Conclusion
Nothing else matters when you are unable to breathe. Efficient COPD management is necessary to improve and sustain quality of life. Severe complications can be prevented if symptoms are discovered early and treatment is commenced. Lifestyle modification is the single most important factor that could greatly improve disease outcomes. In the world today, information and technology have made medicine easier with telemedicine and people can seek medical care promptly.
References
Chronic Obstructive Pulmonary Disease (COPD). (2023, March 16). Retrieved October 24, 2023, from www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd)
Wise, R. A. (2023, October 13). Chronic Obstructive Pulmonary Disease (COPD). Retrieved October 24, 2023, from www.msdmanuals.com/home/lung-and-airway-disorders/chronic-obstructive-pulmonary-disease-copd/chronic-obstructive-pulmonary-disease-copd
Ding, H., Fatehi, F., Maiorana, A., Bashi, N., Hu, W., & Edwards, I. (2019, October 1). Digital Health for COPD Care: The Current State of Play. Retrieved October 24, 2023, from doi.org/10.21037/jtd.2019.10.17
Sorensen, G., Emmons, K., Stoddard, A. M., Linnan, L., & Avrunin, J. (2002). Do social influences contribute to occupational differences in quitting smoking and attitudes toward quitting?. American journal of health promotion: AJHP, 16(3), 135–141. doi.org/10.4278/0890-1171-16.3.135

















