
Prevalence, diagnosis, treatment and management of COPD, by Theresa Lowry-Lehnen
With an estimated 392 million people affected globally, COPD represents a substantial healthcare burden, causing significant morbidity and mortality. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 re-defines COPD as a heterogeneous lung condition characterised by chronic respiratory symptoms (dyspnoea, cough, expectoration and/or exacerbations) due to abnormalities of the airways (bronchitis, bronchiolitis) and/or alveoli (emphysema) that cause persistent, often progressive, airflow obstruction (FEV1/ FVC < 0.7).1,18,19
Historically, COPD has been perceived as a condition largely attributed to tobacco smoking, and exposure to noxious particles or gases, predominantly affecting older males. This perspective is limited and does not encompass the full scope of COPD, which affects both genders equally, and can manifest in individuals of a younger age, and those who have never smoked.
The prevalence of COPD in males and females in developed countries is very similar but some studies suggest more harmful effects of smoking among women.3 Females report more dyspnoea and cough, have a steeper decline in lung function over time, and have worse outcomes than males in terms of hospitalisations, respiratory failure and death.3,4
GOLD 2023 suggests that COPD should be viewed as the ultimate outcome of a continuous and intricate interplay between genetic (G) and environmental (E) factors throughout a person’s lifetime (T). This interplay leads to lung damage and disrupts the natural processes of lung development and ageing.1,18
Risk factors
The most significant genetic risk factor for COPD, although infrequent, arises from mutations in the SERPINA1 gene, which result in α-1 antitrypsin deficiency. Other genetic variants have been identified as risk factors for reduced lung function and COPD, but their individual effect is small.5
Cigarette smoking is a key environmental risk factor; however, fewer than 50 per cent of heavy smokers develop COPD and about a third of patients with COPD have never smoked. COPD in non-smokers is more common in females of younger age.6,7
Passive smoking exposure is a risk factor for COPD, and smoking during pregnancy poses a risk for the foetus, by altering lung growth and development in utero.2 Wood, animal dung, crop residues, and coal (biomass) burned in poorly functioning stoves, may lead to very high levels of household air pollution and increase the risk of COPD.8
Occupational exposures, including organic and inorganic dusts, chemical agents, and fumes, and air pollution also increases the risk.9,10 Other contributing factors include lung growth and development, socioeconomic status, asthma and airway hyper-reactivity, chronic bronchitis, and infections.12
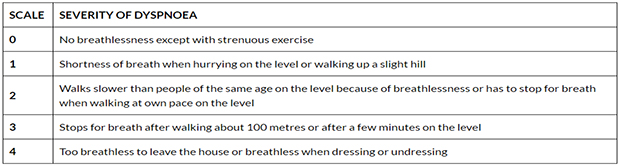
Medical Research Council dyspnoea scale
Clinical presentation and diagnosis
Patients with COPD usually present with symptoms of chronic and progressive dyspnoea, cough, and sputum production, and may also complain of wheezing and chest tightness. The diagnosis of COPD involves a detailed patient history, physical examination, assessment of symptoms, and spirometry. Other investigations may include an FBC and TFTs, an ECG and radiographic imaging (Chest x-ray).11,12
Biomarkers like blood eosinophil count and serum C-reactive protein (CRP) are increasingly used to assess airway inflammation and guide treatment decisions.15
A diagnosis of COPD should be considered in any patient who complains of dyspnoea, chronic cough or sputum production, a history of recurrent lower respiratory tract infections and/or a history of exposure to risk factors.2
Patients should be questioned about their past medical history for conditions such as asthma, allergies, and childhood respiratory infections. Those with liver disease, basilar emphysema, and a family history of emphysema should raise suspicion for alpha-1 antitrypsin deficiency.11
Pulmonary function testing (PFT) is essential in the diagnosis, staging, and monitoring of COPD. The diagnosis is confirmed by spirometry. Spirometry is performed before and after administering an inhaled bronchodilator.
Inhaled bronchodilators may be a short-acting beta2-agonist (SABA), short-acting anticholinergic, or a combination of both. A ratio of the forced expiratory volume in one second to forced vital capacity (FEV1/FVC) less than 0.7 confirms the diagnosis of COPD. Patients with a significantly reduced FEV1 and signs of dyspnoea should be evaluated for oxygenation with pulse oximetry or arterial blood gas analysis.11
The impact of symptoms on patients can be assessed using the COPD assessment tool (CAT) test and the Medical Research Council Dyspnoea (MRC) scale. The CAT test is a validated eight-item measure of health status impairment in COPD, designed to measure the impact of COPD on a person’s life, and how it changes over time.13 The MRC dyspnoea scale is used alongside the questionnaire to establish clinical grades of breathlessness.14
Medical Research Council dyspnoea scale
GOLD 2023 has modified the previous ABCD assessment tool to ABE. The A and B groups remain unchanged, but the former C and D groups are now merged into a single group termed “E” for “Exacerbations”. This aims to recognise the clinical impact of exacerbations, independently of the level of symptoms of the patient.1,18
Treatment and management
The primary goals of COPD treatment are to control symptoms, improve the patient’s quality of life, and reduce exacerbations and mortality. Depending on local guidelines, patients should be offered vaccination against influenza, pneumococcus, Covid-19, pertussis, and herpes zoster.18 Non-pharmacological approaches include smoking cessation and pulmonary rehabilitation.
Comprehensive pulmonary rehabilitation programs, including exercise training, education, and psychological support, remain a cornerstone of COPD management. All COPD patients should be educated about their condition and its treatments, including the correct use of inhalers/devices, and know when to seek help.1,18
Pharmacological interventions are employed to alleviate symptoms, reduce the severity and occurrence of exacerbations, and enhance exercise capacity and overall well-being. Central to the management of stable COPD, bronchodilator therapy continues to play a pivotal role. Regular review of COPD should focus on dyspnoea and exacerbations.1,18
Commonly used medications in COPD include bronchodilators (beta2-agonists, antimuscarinics, methylxanthines), inhaled corticosteroids (ICS), systemic glucocorticoids, phosphodiesterase-4 (PDE4) inhibitors, and antibiotics.
For long-term therapy, the choice of treatment varies and should be tailored to individual patients. Management is largely based on the severity of the disease and symptoms as outlined by GOLD.11
The main groups of COPD medications include:11,12
- Beta-agonists relax smooth muscle by stimulating the beta2 adrenergic receptors. They can be classified into short-acting (SABA) e.g., salbutamol, and long-acting (LABA) e.g., salmeterol, indacaterol, vilanterol, formoterol, and olodaterol.
- Antimuscarinics work by blocking the M3 muscarinic receptors in the smooth muscle, therefore preventing bronchoconstriction. They can be classified into short-acting (SAMA) e.g., ipratropium and long-acting (LAMA) e.g., tiotropium, umeclidinium, aclidinium bromide, and glycopyrronium.
- Combining bronchodilators may increase the degree of bronchodilation and lower the risk of side-effects compared to increasing the dose of a single bronchodilator agent.
- Methylxanthines provide evidence of bronchodilation in stable COPD but remain controversial regarding their mechanism of action. Theophylline is the most used methylxanthine, however, there are significant drug interactions with its use and clearance of the drug declines with age.
- Inhaled corticosteroids (ICS): ICS are not recommended in patients with <100 Eos/μL. The use of LABA + ICS in COPD is no longer encouraged. If there is an indication for an ICS, then LABA + LAMA + ICS has been shown to be superior to LABA + ICS and is therefore the preferred choice.18
Phosphodiesterase-4 inhibitors work by inhibiting the breakdown of intracellular cyclic AMP, therefore reducing inflammation. Roflumilast is a PDE4 inhibitor; a non-steroid, anti-inflammatory active substance designed to treat both the systemic and pulmonary inflammation associated with COPD.11
Systemic glucocorticoids in COPD exacerbations improve lung function, oxygenation, risk of early relapse, and reduce treatment failures and length of hospitalisation.18
Antibiotics should be given to patients with ECOPD who have increased sputum volume and sputum purulence. The recommended length of antibiotic therapy is 5-7 days, and choice based on the local bacterial resistance pattern.18
Triple Therapy: Inhaled corticosteroids (ICS), long-acting beta-agonists (LABA), and long-acting muscarinic antagonists (LAMA) as a triple therapy have gained prominence in managing moderate to severe COPD. Recent trials have shown that triple therapy can improve lung function, reduce exacerbations, and enhance quality of life.16
Emerging biologic therapies targeting specific inflammatory pathways, such as anti-IL-5 (e.g., mepolizumab) and anti-IL-4/IL-13 (e.g., dupilumab), are being investigated in COPD. These biologics offer hope for patients with severe eosinophilic and allergic phenotypes.17 ![]()
Key headlines for GOLD pharmacological treatment recommendations of COPD18
(www.goldcopd.org)
- For symptomatic patients, a LABA-LAMA therapy in a single inhaler is recommended as initial therapy.
- The continuance of LABA-ICS is no longer recommended in patients with COPD.
- Triple therapy (LABA-LAMA-ICS) is recommended in COPD patients who still suffer exacerbations of the disease despite LABA-LAMA therapy, if blood Eosinophil levels are higher than 100 cells /μL.
- ICS are not recommended in patients with <100 Eos/μL.
- Pharmacologic treatment must always be combined with non-pharmacologic treatment (including adequate treatment compliance, smoking cessation, physical activity and appropriate vaccination), and consideration of coexistent comorbidities.
References available upon request.
Author
Theresa Lowry Lehnen, RGN, PG. Dip Coronary Care, RNP, BSc, MSc, PG. Dip. Ed (QTS), M. Ed, PhD, Clinical Nurse Specialist and Associate Lecturer South East Technological University.

















