
Improved monitoring on low-acuity wards needs to be practised in a structured way. This article provides an example of how standardised monitoring platforms can aid the application of clinical judgement
Table of Contents
Abstract
The National Early Warning Score 2 (NEWS2) is a robust, evidence-based tool that enables health professionals to recognise deterioration in a patient and understand when it is appropriate to escalate their care. This article reminds nurses of the synonymous relationship between the NEWS2 chart and the airway, breathing, circulation, disability, exposure (ABCDE) approach to assessing and treating patients who are acutely unwell, illustrating how both can work together to enable early recognition in a patient who is suspected of deteriorating, despite a low-risk aggregate score. The article uses a fictitious clinical scenario to demonstrate this approach to assessment.
Citation: Eakins F (2022) Preventing deterioration before a NEWS2 score is triggered. Nursing Times [online]; 118, 7.
Author: Freya Eakins is intensive care nurse, Hywel Dda University Health Board.
- This article has been double-blind peer reviewed
- Scroll down to read the article or download a print-friendly PDF here (if the PDF fails to fully download please try again using a different browser)
Introduction
A fundamental requirement of all competent nurses is the ability to recognise deterioration in a patient and understand when it is appropriate to escalate. The universal ‘track-and-trigger’ system of the National Early Warning Score (NEWS) – whereby a score is allocated to six physiological measurements – is widely used as a robust, evidence-based tool to aid health professionals in this process. In December 2017, NEWS was updated to National Early Warning Score 2 (NEWS2) to address shortfalls identified in its original model. A prescribed scale for safe oxygen use for patients with hypercapnic (type-2) respiratory failure was added; this and other refinements aimed to identify people at risk of new serious deterioration (Royal College of Physicians (RCP), 2017). Through standardisation of NEWS2, it is estimated that more than 1,800 patient lives are saved each year (NHS, nd).
Despite these encouraging statistics, it is worth asking whether the emphasis on clinical judgement has been lost along the way. In the UK, all registered nurses are expected to conduct a whole-body systems assessment, as well as interpret these findings, as part of the requirement for the Nursing and Midwifery Council (NMC)’s (2018) proficiency standards for registered nurses. In 2019, Jensen et al’s qualitative study of hospital nurses’ perceptions of, and reactions to, track-and-trigger systems identified four central barriers to their use; these were problems with:
- Community of practice;
- Rules and compliance;
- Division of labour;
- Using standardised tools and misrepresentation of clinical judgement.
These barriers invariably affect nurses’ compliance and competence in using track-and-trigger systems appropriately.
This article challenges perspectives on NEWS2, by highlighting how practitioners can use their comprehensive knowledge of physiology and assessment in partnership with patient collaboration – through interaction, observation, intervention and employed technology – to improve clinical accuracy and patient outcomes.
Standards and frameworks
In the UK, the National Institute for Health and Care Excellence (NICE), the Care Quality Commission (CQC), and the National Patient Safety Agency recognise the need to ensure patients are safe, and prioritise the development of standards and frameworks that prompt recognition of deterioration. The use of NEWS2 as a quality indicator has been recorded by the CQC during hospital inspections and evaluated to improve both patient outcomes and mortality rates (RCP, 2017). Despite these provisions, evidence suggests the response to the deteriorating patient is still of ongoing concern (Burke et al, 2020). Irrespective of widespread implementation of track-and-trigger systems, in 2019, 63.7% of avoidable deaths were attributed to preventable conditions in England; the figure was 62.8% for Wales (Office for National Statistics, 2021). Clinical research shows patient deterioration is often detected late or missed completely, contributing to the development of serious adverse events (Petersen Tym et al, 2017).
Although much research has sought to explore the nurse’s role in recognising clinical deterioration, there has been little exploration of the causes of failure-to-rescue rates; in the qualitative data that does exist, the causes that emerge are a lack of knowledge and educational resources available to registered nurses predominantly working in level-1 inpatient settings (Chua et al, 2019). The implementation of early-warning scoring systems is only effective if nurses can recognise and act on clinical deterioration in a timely manner. Evidence shows that physiological knowledge, clinical judgement and person-centred decision-making are needed to improve in-hospital mortality rates (Chua et al, 2019).
The main aim of NEWS2 is to embed a cultural shift in the NHS by making health professionals more aware of when it is appropriate to respond, escalate and transfer to a higher dependency of care. This approach to deterioration – sometimes referred to as the ‘three Rs’ – recognise, relay, react – has been found effective in reducing failure-to-rescue rates (Burke et al, 2020). Adopting a complication-management approach can mitigate unidentified deterioration by creating an intuitional competence in this context.
A NEWS2 score of ≥5 is:
- Classified as a key threshold for urgent response;
- Associated with mortality rates three times higher than those of a NEWS2 score of 0-4 (RCP, 2017).
Translating the aggregate scoring system into patient outcomes sets a clear precedent for the importance of using independent thought and clinical reasoning when performing observational checks. If each NEWS2, irrespective of the level of risk, was used in conjunction with a subjective and qualitative tool – such as the Resuscitation Council UK’s (RCUK) airway, breathing, circulation, disability and exposure (ABCDE) approach to the assessment of critically ill patients – nurses would be able to predict early deterioration hours before abnormal vital signs (Table 1) are displayed.

What can be missed using NEWS2?
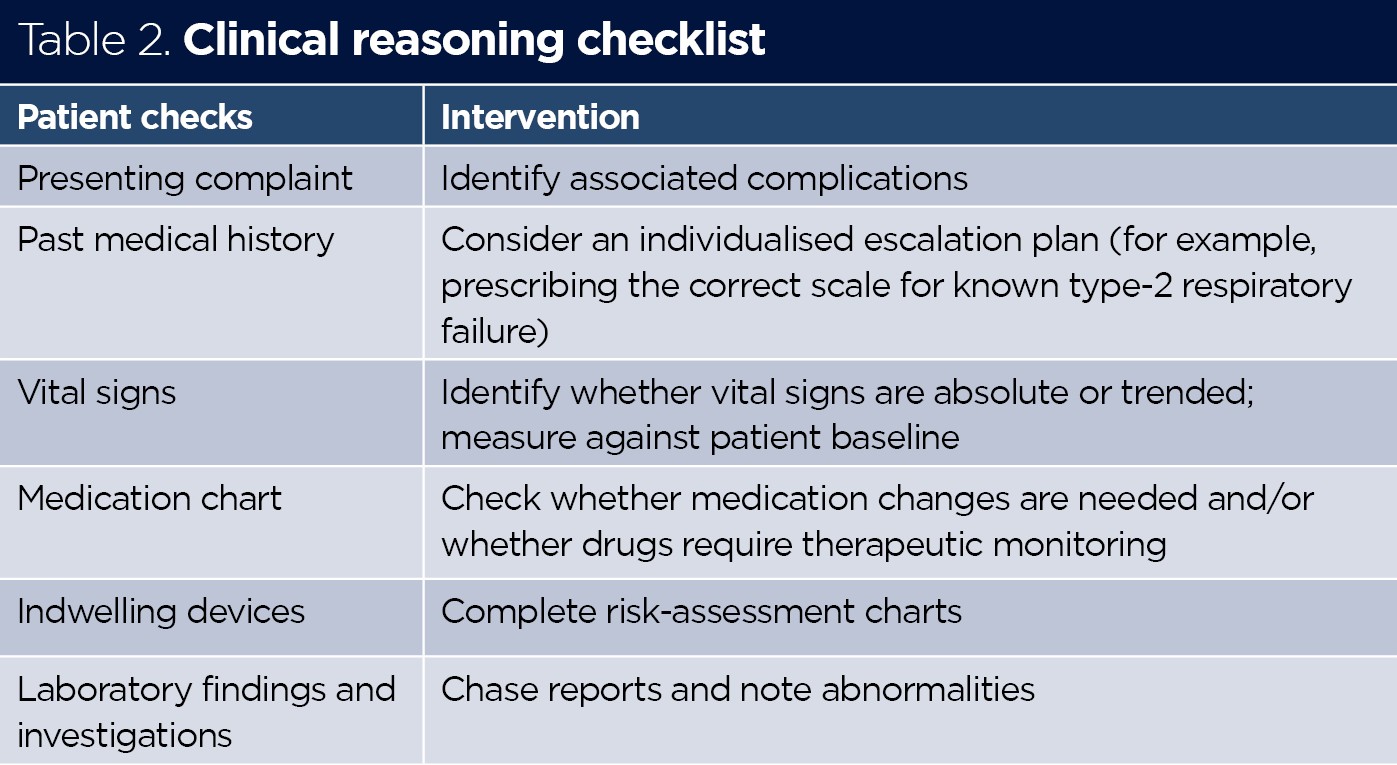
The RCP (2017) highlighted that track-and-trigger systems carry many contentions so should not be a substitute for competent clinical assessment. Irrespective of the NEWS2 score, any concern about the stability of a patient’s condition should prompt thorough clinical assessment and review. Taking observations is not just about generating numbers and activating the specific escalation pathway according to the aggregate score; it is knowing the patient’s diagnosis, comorbidities, associated complications and management plan. A clinical reasoning checklist is given in Table 2.
Box 1 details a fictitious scenario of a patient (Mr Jones) whose deterioration could have been identified earlier if a focused bedside-assessment tool, such as the ABCDE approach, had been used. Understanding the associated risks and cardinal signs of each individual patient’s comorbidities can help with the direction and emphasis of the clinical assessment.
Box 1. Sample scenario
Mr Jones, aged 76 years, was admitted to a general medical ward three days after presenting to the emergency department with fatigue, chest pain and exertional breathlessness. An electrocardiogram showed he was in AF so he was admitted for further investigations and heart rate control. He has a past medical history of ischaemic heart disease, chronic obstructive pulmonary disease and hypertension. Since starting treatment for the AF, his heart rate has been controlled and, reportedly, his symptoms have improved.
On arrival at the ward, Mr Jones is alert and orientated, but reports having had a restless night due to breathlessness. These are his vital signs:
- Respiratory rate: 20 breaths per minute
- Oxygen saturation: 93% on room air
- Heart rate: 89 beats per minute
- Blood pressure: 137/73
- Temperature: 36.5°C
His NEWS2 score at 9am is 0 and he is classified as low risk. A lower target of 88-92% oxygen saturation is indicated for his hypercapnic respiratory failure on the NEWS2 chart for scoring oxygen saturation; this decision should be made by a competent clinical physician – usually the specialty registrar – and recorded in the patient’s medical notes.
At midday, Mr Jones calls his bell for attention; he is only able to speak in short sentences and is extremely dyspnoeic. These are now his vital signs:
- Respiratory rate: 28 breaths per minute
- Oxygen saturation: 86% on room air
- Heart rate: 120 beats per minute
- Blood pressure: 168/78
- Temperature: 36.7°C
His NEWS2 score is now 6 and requires an urgent response. This means commencing hourly monitoring of vital signs (as a minimum) and immediately requesting a review by a clinician or team competent in acutely ill patients.
AF = atrial fibrillation; NEWS2 = National Early Warning Score 2
The following sections explore an integrated, patient-specific assessment based on the NEWS2 chart and Mr Jones’ presenting complaint.
Airway
The assessment of Mr Jones’ airway is patent and secure; this is confirmed by his ability to speak in sentences with normal tone. However, the ‘look, listen, feel’ assessment tool is paramount when identifying risk factors of a potentially unprotected airway. The aim of the airway assessment is to identify any obstruction, whether complete or partial.
In partial obstruction, the patient may look agitated, have increased accessory muscle use and be gasping for air. Noisy breath sounds, particularly gurgling sounds, are indicative of a partially occluded airway (Sampson, 2021). The character of the noise provides an indication of the location and cause of the obstruction; in complete airway obstruction there are no breath sounds at the mouth or nose. Looking at the patient, you may see a paradoxical (‘see-saw’) breathing pattern; use of the accessory muscles, pallor or cyanosis are late signs.
The main causes of airway obstruction are:
- Foreign bodies;
- Allergic reaction;
- Laryngeal oedema;
- Pooled secretions;
- Tongue displacement;
- Reduced consciousness (Webb et al, 2016).
If a completely obstructed airway is suspected, look inside the mouth for signs of airway obstruction, observe the chest for adequate rise and fall and bilateral chest expansion, and listen for the presence of breath sounds; no air entry at auscultation or high-pitched breathing noises (stridor) are all signs of complete airway obstruction (Heuer, 2021).
Airway obstruction is an emergency. Expert help should be sought immediately, and the airway should be opened using the head-tilt/chin-lift manoeuvre. Untreated, airway obstruction causes hypoxia and risks damage to the brain, kidneys and heart, as well as cardiac arrest and death (RCUK, nd).
Mr Jones has a history of type-2 respiratory failure; this means a target saturation must be prescribed to determine the most appropriate scale on the oximetry section of the NEWS2 chart. Consider referring to previous records for a last-recorded oxygen saturation and asking the patient what is normal for them. Is 93% consistent with what has previously been recorded? Best practice is prescribing a target range for all hospital patients at the time of admission, so that appropriate oxygen therapy can be started in the event of unexpected clinical deterioration (O’Driscoll et al, 2017).
In the event of hypoxaemia, where a target saturation has not been prescribed and the patient’s history is unknown, acute respiratory failure should be assumed and 15L oxygen should be provided via a high-flow, non-rebreather reservoir mask (RCUK, nd).
If new hypoxaemia is suspected in Mr Jones, the airway should be assessed for partial obstruction. This would cause air entry to be diminished and often noisy; simple methods of airway clearance and suctioning can remove pooled secretions (Peate and Dutton, 2021).
The British Thoracic Society’s emergency-oxygen guideline – O’Driscoll et al (2017) – recommends oxygen saturations of 88-92% in patients admitted with exacerbations of chronic obstructive pulmonary disease (COPD). This must be confirmed following the guidance of a clinician, based on the NEWS2 guidelines (RCP, 2017). Some patients with chronic lung disease carry an oxygen alert card that documents their target saturation. High concentrations may depress breathing in a subgroup of patients with COPD, leading to an increased risk of airway obstruction (RCUK, nd).
Breathing
The respiratory system adapts readily to demands placed on it, and early identification of changes in respiratory rate can facilitate prompt treatment. The RCUK (nd) recommends that respiratory assessment follows a logical, structured approach. There are four main components to comprehensive respiratory assessment:
- Inspection;
- Palpation;
- Percussion;
- Auscultation (Morgan, 2021).
To assess the stability of respiratory function, it is important to observe the patient’s work of breathing from a distance. Observation should include pattern, depth and regularity of breathing, as well as checking whether there is use of the sternocleidomastoid, scalene or pectoralis minor muscles and whether the patient is pursing their lips or flaring their nostrils (Wheatley, 2018).
Assessing Mr Jones’ colour and checking his skin, nail beds and mucous membranes for pallor or cyanosis would provide information about his perfusion (Gulanick and Myers, 2011). Observing the position he is in could also indicate his respiratory effort; for example, a high Fowler’s position allows for increased respiratory capacity and full descent of the diaphragm. Simply asking Mr Jones how well he slept or observing the number of pillows used could reveal an early precursor to the change in his condition from baseline (Cooper and Gosnell, 2019).
When Mr Jones’ respiratory effort increases from baseline, checking the trend from previous recordings would indicate whether a respiratory rate of 20 is normal for him; a subtle change might be noticed. While counting a patient’s respiratory rate over one minute, you should be assessing the depth of each breath, the pattern, the rhythm of respiration and whether chest expansion is equal on both sides. When the rate of breathing has been determined, consider whether this is normal for the patient and use their trend as a guide to aid your clinical judgement. Patients adapt their breathing pattern over time to facilitate gas exchange. In the early stages of compensation, there is a mild increase in respiratory rate and, as the underlying cause progresses, so does the dyspnoea.
After gaining consent, a physical examination of the chest wall can also help identify any abnormalities in respiratory function that may have been missed. Note whether there are any anterior or posterior chest wall deformities. To feel for symmetry, place your hands on either side of the patient’s anterior chest with your thumbs touching at the second intercostal space and ask the patient to inhale deeply; your thumbs should separate equally, several centimetres away from the sternum (Potter, 2021).
If asymmetry is suspected, palpate the patient’s trachea for deviation; the trachea should be anatomically medial to the ends of the clavicle and central to the suprasternal notch. If a trachea deviates, it will deviate to the direction of less pressure, away from a collapsed lung (Lister et al, 2020). Asymmetrical chest movement and tracheal deviation can indicate underlying conditions such as large pneumothorax, pleural effusion and rib fractures (Innes, 2018). New tracheal deviation is an emergency: help must be summoned immediately. Asymmetrical chest movements require an urgent review by the medical team.
When feeling for symmetry and observing work of breathing, listen to the patient’s breath sounds and note the pattern. Signs requiring further assessment in palpation include:
- A paradoxical (see-saw) breathing pattern;
- Hyperinflation on chest expansion;
- Adventitious or abnormal breath sounds, such as a wheeze.
If these signs are present, you could palpate for tactile or vocal fremitus by feeling the vibrations produced when the patient speaks or uses percussion. Dullness indicates fluid or consolidation in lung fields; hyperresonance indicates air in the pleural cavity, suggesting a pneumothorax (Crouch et al, 2016).
If the health professional is competent in performing auscultation, the procedure can provide further clinical evidence to support the findings of an abnormal breathing assessment. Normal breath sounds are tracheal, bronchial, bronchovesicular and vesicular, depending on where they are heard (Ball et al, 2021). Patients with noisy breath sounds should be assessed for their ability to expectorate: assess what their sputum load is, along with its colour and consistency if they have a productive cough.
Circulation
Cardiovascular disease remains one of the leading causes of death worldwide (Mladenka et al, 2018), so it is essential that nurses possess a comprehensive understanding of cardiovascular anatomy and physiology. The cardiovascular system is complex, comprising the heart and an extensive network of blood vessels that extend into two anatomically separate systems:
- Pulmonary circulation system (lungs);
- Systemic circulation system (body).
Each subordinate organ has a multifaceted role in regulating homeostasis (Creed and Spiers, 2020).
The heart is a unique organ because it is autorhythmic (Colman and Holden, 2019): its specialist conduction system means it self-regulates and produces no downtime. The limitation of this circuit means multiple problems – for example, cardiovascular pathologies, physiological disturbances or drug-induced cardiotoxicity – can impair it or threaten its electrophysiology (Mladenka et al, 2018). The rate, rhythm and strength of the pulse indicate how well the heart is working.
Assessing the regularity of pulsations helps determine the presence of cardiac arrythmias (Peate et al, 2014). Mr Jones’ atrial fibrillation (AF) provides a baseline rate, strength and rhythm. In all known cardiac arrhythmias, the pulse should be assessed manually, rather than via a pulse oximeter, as an abnormal heart rhythm such as with AF will provide an inaccurate reflection in ventricular rate, regularity and strength (Alagappan, 2018). The rhythm should be assessed and noted to prevent unidentified change; abnormally weak or strong pulses suggest abnormal stroke volumes (Hajar, 2018).
If a weak and thready pulse is palpated, observe the patient’s colour, digit temperature and capillary refill time for prolongation (>2 seconds). Each of these observations can reveal a lack of perfusion. The body initially compensates for the reduced cardiac output through subtle changes, usually only identifiable by a prolonged capillary refill time, pallor and changes in skin temperature. Pale, cyanosed or mottled peripheries are poorly perfused; abnormally warm or flushed peripheries indicate excessive dilation from distributive shock (Hariri et al, 2019).
When observing limbs, assess for the presence of peripheral oedema by palpating the areas over the tibia, ankles and feet. If peripheral oedema is present, documenting the level to which it extends on admission will allow the assessor to see whether things improve. The development of peripheral oedema in heart failure is related to fluid excess: as the heart fails, renal perfusion diminishes, which is followed by sodium and water retention (Pellicori et al, 2015).
If fluid retention is suspected, check for an accurate record of fluid intake and output over the previous 24 hours and calculate the fluid deficit. If the patient is showing positive signs of fluid retention, their current weight should be compared with their admission weight; body weight is a more sensitive indicator of fluid retention (Davies et al, 2015).
Disability
An initial assessment of disability should be measured by the patient’s level of consciousness, using the alert, confusion, voice, pain, unresponsive (ACVPU) scale. This scale is quick, simple and helpful for making a rapid assessment of a person’s gross level of consciousness or mental state (Romanelli and Farrell, 2021). The assessment is completed in sequence and the person’s response is recorded in order of appropriateness, based on the nurses’ initial awareness of the patient’s consciousness:
- A – the patient is fully alert with eyes open and cognisant;
- C – confusion and changes in neurological state: these are significant and often indicate signs of deterioration well before other parameters change;
- V – the patient responds to voice, then closes their eyes again until next stimulated by verbal stimuli with evident drowsiness;
- P – the patient only responses when pain is inflicted (trapezium pinch or sternal rub);
- U – unresponsive to pain (Barker, 2019).
Any deviation from alert (A) should prompt a more in-depth assessment to be performed. The Glasgow Coma Scale (GCS) is considered the gold standard in the UK and is the tool generally used by nurses to assess neurological function (Steen et al, 2021). Similar to the ABCDE approach, it requires nurses to establish whether the level of consciousness and cognitive state are normal for the patient. A normal GCS score is 15/15, but the GCS baseline may be lower in some patients with dementia, underlying chronic neurological disorders or learning disabilities. This should always be confirmed by someone who is involved in the patient’s care and competent to make this decision (NICE, 2014).
A patient with a GCS score of <15 on initial assessment should be reviewed for indicators of neurological compromise. Look for pupil size, equality and reaction to light. Normal pupil size is 2-5mm and reaction to light should be brisk. Following removal of the light source, the pupil should return to its original size; this response should be consensual in both eyes (Jevon, 2016). Pupillary reaction assesses the third cranial nerve (oculomotor nerve) – an abnormal pupil reaction, size or shape is an indicator of raised intracranial pressure (Goulden and Clarke, 2016).
A patient who scores P or U on the ACVPU scale is considered to have a GCS score of ≤8 and, therefore, the airway is unprotected (Romanelli and Farrell, 2021). These patients should always be nursed in a lateral position to maintain patency before urgent review by the medical team or anaesthetist. Causes of the change in mental status should always be investigated, as these may be multifactorial.
If medication changes have recently been made, the medication chart should be reviewed for drugs such as opioids, benzodiazepines, neuroleptic drugs or over-oxygenation in hypercapnic respiratory failure. The blood–glucose level should also be measured to exclude hypoglycaemia. If capillary blood sugars are <4mmol/L, follow local protocols for the treatment of hypoglycaemia (RCUK, nd).
Exposure
The exposure assessment is the final process and can help solidify a nursing diagnosis or identify a cause of deterioration. In Mr Jones’ case, his temperature should first be recorded to make sure it is in the normal range; the accepted value for NEWS2 is 36.1-38.0°C. A thorough head-to-toe examination should then be undertaken to identify any:
- Broken areas to skin;
- Injuries;
- Oedema;
- Venous thromboembolism;
- Evidence of external and/or internal bleeding.
The site of any indwelling catheters, drains and peripheral vascular-access devices should also be checked for clinical signs of infection, such as rashes, skin changes or phlebitis, using the visual infusion phlebitis score (Dutton and Finch, 2018).
When assessing exposure, it is important to consider skin integrity. The risk of pressure sores is greater because of Mr Jones’ reduced exercise tolerance. Skin integrity should be considered using tools related to organisation and, depending on the level of risk and professional discretion, the appropriate interventions should be undertaken.
Conclusion
Nurses have a fiduciary responsibility and are under increasing pressure to keep up to date with changes in society and healthcare. What patients require from nurses is becoming more complex, as new proficiencies, standards and autonomous roles in nursing arise, so it is important to make quality of care more efficient and timely. Early identification of patient deterioration can be achieved without increasing nurses’ workload by combining two effective assessments. Incorporating a whole-body assessment into routine standardised framework tools will improve failure-to-rescue rates. In-hospital mortality rates can be reduced by making use of physiological knowledge, clinical judgement and person-centred decision-making; the application of all three must be integrated into staff recruitment, training and the institutional culture to improve patient outcomes.
Key points
- Incorporating a whole-body assessment into standardised framework tools will improve failure-to-rescue rates
- Early identification of patient deterioration can be achieved by combining two systematic assessments: the National Early Warning Score 2 and the airway, breathing, circulation, disability, exposure (ABCDE) approach
- It is important to use independent thought and clinical reasoning when performing observational checks
- A person-centred approach to care of the deteriorating patient is vital
Alagappan R (2018) Manual of Practical Medicine. Jaypee Brothers Medical Publishers.
Ball JW et al (2021) Seidel’s Guide to Physical Examination: An Interprofessional Approach. Elsevier.
Barker S (2019) Intermediate life support for the adult. British Journal of Nursing; 28: 4, 226-228.
Burke JR et al (2020) Failure to rescue deteriorating patients: a systematic review of root causes and improvement strategies. Journal of Patient Safety; 18: 1, e140-e155.
Chua WL et al (2019) Seeing the whole picture in enrolled and registered nurses’ experiences in recognizing clinical deterioration in general ward patients: a qualitative study. International Journal of Nursing Studies; 95: 56-64.
Colman MA, Holden AV (2019) Modeling the heart. In: Roberts G et al (eds). Encyclopaedia of Biophysics. Springer
Cooper K, Gosnell K (2019) Foundations and Adult Health Nursing. Mosby.
Creed F, Spiers C (2020) Care of the Acutely Ill Adult. Oxford University Press.
Crouch R et al (2016) Oxford Handbook of Emergency Nursing. Oxford University Press.
Davies H et al (2015) Effectiveness of daily fluid balance charting in comparison to the measurement of body weight when used in guiding fluid therapy for critically ill adult patients: a systematic review protocol. JBI Database of Systematic Reviews and Implementation Reports; 13: 3, 111-123.
Dutton H, Finch J (2018) Acute and Critical Care Nursing at a Glance. Wiley Blackwell.
Goulden I, Clarke D (2016) Traumatic brain injury. In: Clarke D, Malecki-Ketchell A (eds) Nursing the Acutely Ill Adult: Priorities in Assessment and Management. Palgrave.
Gulanick M, Myers JL (2011) Nursing Care Plans: Diagnoses, Interventions, and Outcomes. Mosby.
Hajar R (2018) The pulse from ancient to modern medicine: part 3. Heart Views; 19: 3, 117-120.
Hariri G et al (2019) Narrative review: clinical assessment of peripheral tissue perfusion in septic shock. Annals of Intensive Care; 9: 37.
Heuer AJ (2021) Wilkins’ Clinical Assessment in Respiratory Care. Elsevier.
Innes JA (2018) Macleod’s Clinical Examination. Elsevier.
Jensen JK et al (2019) Introducing the National Early Warning Score: a qualitative study of hospital nurses’ perceptions and reactions. Nursing Open; 6: 3, 1067-1075.
Jevon P (2016) Clinical Examination Skills. Wiley.
Lister S et al (2020) The Royal Marsden Manual of Clinical Nursing Procedures. Wiley.
Mladěnka P et al (2018) Comprehensive review of cardiovascular toxicity of drugs and related agents. Medicinal Research Reviews; 38: 4, 1332-1403.
Morgan S (2021) Respiratory assessment: undertaking a physical examination of the chest in adults. Nursing Standard; 37: 3, 75-82.
National Institute for Health and Care Excellence (2014) Head Injury: Assessment and Early Management. NICE.
NHS (nd) News Early Warning Score (NEWS). england.nhs.uk (accessed 27 May 2022).
Nursing and Midwifery Council (2018) Future Nurse: Standards of Proficiency for Registered Nurses. NMC.
O’Driscoll BR et al (2017) BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax; 72: ii1-ii90.
Office for National Statistics (2021) Avoidable mortality in the UK: 2019 – deaths from causes considered avoidable, treatable or preventable given timely and effective healthcare or public health interventions. ons.gov.uk, 26 February (accessed 14 June).
Peate I et al (2014) Nursing Practice: Knowledge and Care. Wiley Blackwell.
Peate I, Dutton H (2021) Acute Nursing Care: Recognising and Responding to Medical Emergencies. Routledge.
Pellicori P et al (2015) Fluid management in patients with chronic heart failure. Cardiac Failure Review; 1: 2, 90-95.
Petersen Tym MK et al (2017) Developing models to predict early postoperative patient deterioration and adverse events. ANZ Journal of Surgery; 87: 6, 457-461.
Potter L (2021) Respiratory examination: OSCE guide. geekymedics.com (accessed 27 May 2022).
Resuscitation Council UK (nd) The ABCDE approach. resus.org.uk (accessed 16 March).
Romanelli D, Farrell MW (2021) AVPU Score. StatPearls.
Royal College of Physicians (2017) National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. RCP.
Sampson M (2021) A guide to airway management. British Journal of Cardiac Nursing; 16: 3, 1-13.
Steen C et al (2021) Critical care related to the cardiac system. In: Freeman S et al (eds) Essentials of Nursing Critically Ill Adults. SAGE.
Webb A et al (2016) Oxford Textbook of Critical Care. Oxford University Press.
Wheatley I (2018) Respiratory rate 4: breathing rhythm and chest movement. Nursing Times; 114: 9, 47-48.

















